2096
Whole-Tumor Quantitative Apparent Diffusion Coefficient Histogram Analysis in Differentiating intrahepatic mass-forming cholangiocarcinoma from poorly differentiated hepatocellular carcinoma1Department of Radiology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wu han, People's Republic of China
Synopsis
Differentiating intrahepatic mass-forming cholangiocarcinoma (IMCC) and poorly differentiated hepatocellular carcinoma(pHCC) is often difficult for radiologists, but it is important for providing appropriate treatments. In our study, we use noncontrast MRI with diffusion-weighted imaging in combination with whole-tumor quantitative apparent diffusion coefficient (ADC) histogram analysis to differentiate IMCC from pHCC. The result reveals that ADC histogram analysis based on the whole-tumor can be considered a useful and noninvasive method to help differentiate IMCC from pHCC. Especially ADC25% of histogram analysis allows differentiation of IMCC from pHCC with higher accuracy.
Purpose
To evaluate the value of whole-tumor quantitative apparent diffusion coefficient (ADC) histogram analysis for differentiation of intrahepatic mass-forming cholangiocarcinoma (IMCC) and poorly differentiated hepatocellular carcinoma(pHCC).Introduction
Differentiating IMCC from pHCC is often difficult for radiologists, but it is important for providing appropriate treatments. Surgical resection is the mainstay for treatment of IMCC, while for pHCC, there are a variety of effective means for selection, such as: radiofrequency ablation, percutaneous ethanol injection, trans catheter arterial chemoembolization and so on. Previous studies in regard to the differentiation of IMCC and pHCC in images were mainly studies used contrast media.1,2,3 However, for patients with renal insufficiency, or allergy to contrast media, dynamic enhancement is not suitable. Here we try to explore the value of noncontrast magnetic resonance imaging(MRI) with diffusion-weighted imaging(DWI) in combination with whole-tumor quantitative ADC histogram analysis for differentiating IMCC from pHCC.Methods
Abdominal MRI of 25 patients with IMCC and 13 patients with pHCC whom were confirmed with pathology were retrospectively reviewed. All the patients were performed routine abdominal MRI and DWI(b=0, 800 s/mm2) at 3T. The mean interval between the MRI and surgery or biopsy was 8 days (range 1–42 days) for patients with IMCC, and 5 days (range 2–14 days) for patients with pHCC. The whole-tumor ADC assessments were performed with software (Firevoxel, https://files.nyu.edu/hr18/public/projects.html) on all slices of the tumor to obtain histogram parameters, including the ADCmean, ADCmedian, ADC10%, ADC25%, ADC75%, ADC90%, entropy, skewness and kurtosis. Multiple receiver operating characteristic (ROC) curves analysis was used to determine and compare the diagnostic value of each significant parameter.Results
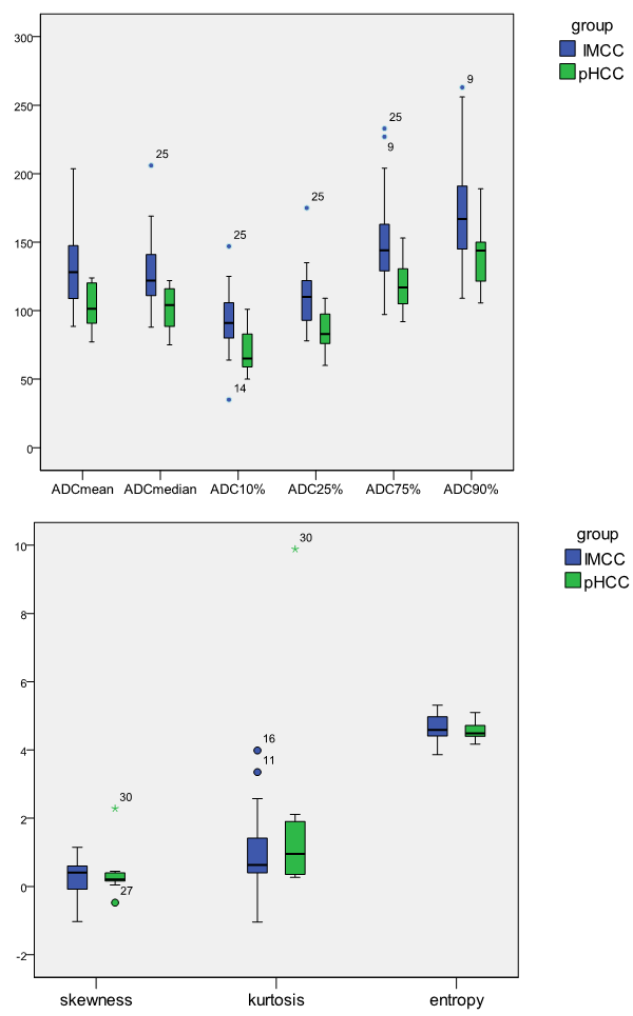
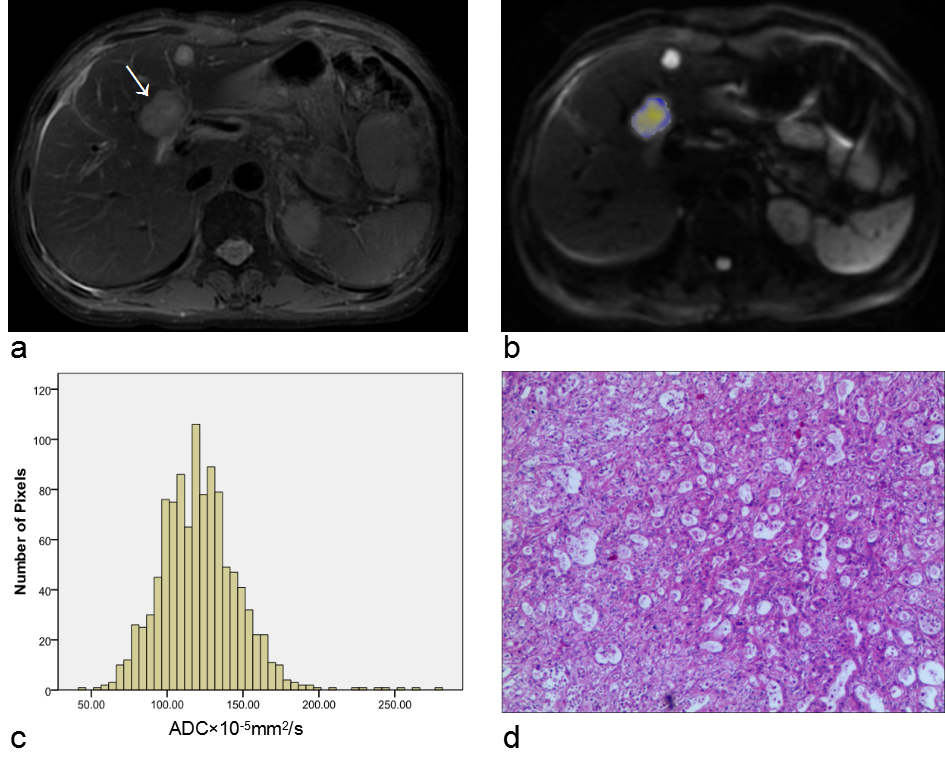
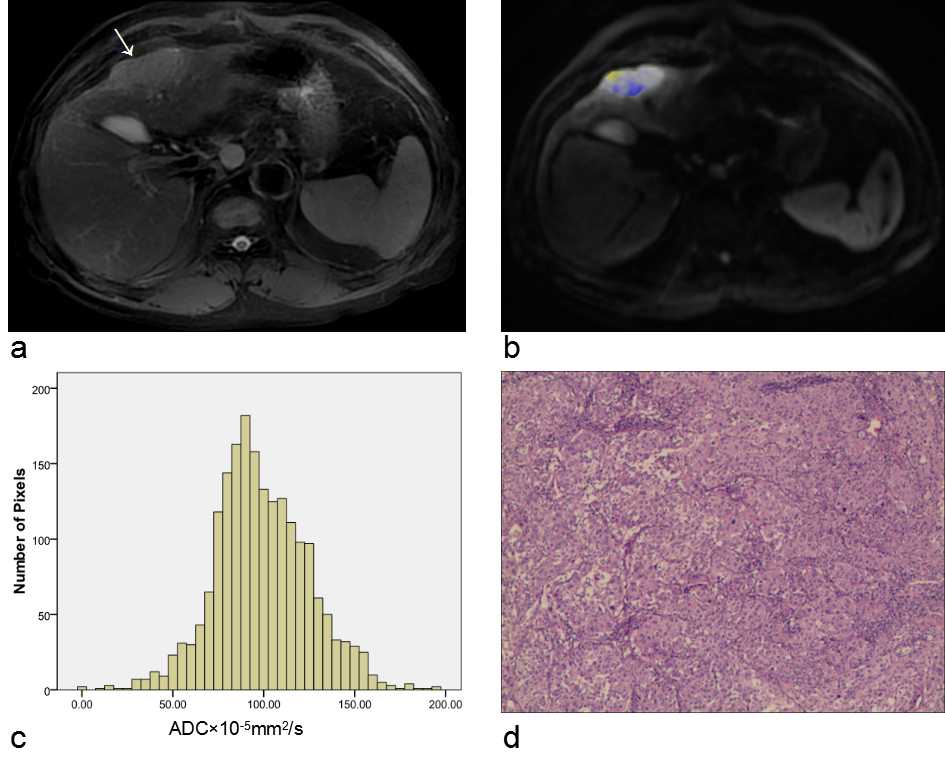
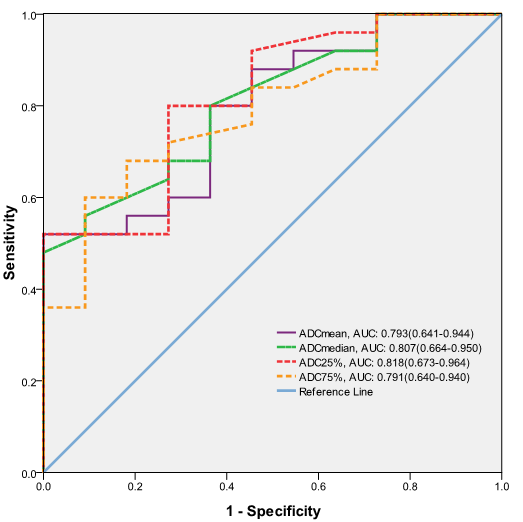
IMCC had significantly higher ADCmean, ADCmedian, ADC10%, ADC25%, ADC75%, and ADC90% than pHCC (P=0.005, P=0.004, P=0.013, P=0.004, P=0.010, P=0.019, respectively)(Fig. 1). No significant difference was observed in the entropy, skewness and kurtosis (P=0.571, P=0.577, P=0.210,respectively). Examples were shown in Fig. 2 and Fig. 3. During ROC curves analysis(Fig. 4), the ADC25% value generated the highest AUC for differentiating IMCC from pHCC (area under the ROC curve(AUC), 0.818; Sensitivity, 80%; Specificity, 72.7%; cut-off value, 0.915×10-3 mm2/s), followed by ADCmedian (AUC, 0.807; Sensitivity, 48%; Specificity, 100%; cut-off value, 1.265×10-3 mm2/s).Discussion
In present study, the preliminary data demonstrate that, ADC histogram parameters, except the entropy, skewness and kurtosis, are helpful in the differential diagnosis of IMCC and pHCC. The whole-tumor ADC histogram analysis represents a texture-based statistical measure of the variation and frequency of ADC values within a given tissue. Whole-tumor analysis method which contains all voxels on all slices of tumor can provide more information compared with focusing on a limited tumor area, such as the largest cross-sectional area.4,5 The whole-tumor ADC histogram analysis may become an effective method of overcoming overlapping ADC values between tumors. In our study, ADC values of IMCC were higher than those of pHCC. We suspect that several factors influence the discrepant results. First, IMCC is more prone to be necrosis in the central area and the necrotic components would yield high ADC values. Second, in most cases, the carcinoma cells of IMCC proliferate in a compact pattern in the peripheral areas, whereas they proliferate sparsely with abundant fibrous stroma in the central area. The fibrous stroma would also yield high ADC values. Besides, to avoid the effects of image artifacts and distortions, the whole lesion with 3D ROIs was slightly smaller than the actual lesion volume, the marginal area of the tumor was not included. Selection bias is unavoidable because of the retrospective nature of our study. In addition, more cases need to be studied.Conclusion
ADC histogram analysis based on the whole-tumor can be considered a useful and noninvasive method to help differentiate IMCC from pHCC. Especially ADC25% of histogram analysis allows differentiation of IMCC from pHCC with higher accuracy.Acknowledgements
We thank Haojie Li, Hao Yu, Anqin Li, and Di Zhu, for their important contributions to this study.References
[1]Kim R, Lee JM, Shin C, et al. Differentiation of intrahepatic mass-forming cholangiocarcinoma from hepatocellular carcinoma on gadoxetic acid-enhanced liver MR imaging. Eur Radiol. 2016;26(6):1808-1817.
[2]Choi SH, Lee SS, Kim SY, et al. Intrahepatic Cholangiocarcinoma in Patients with Cirrhosis: Differentiation from Hepatocellular Carcinoma by Using Gadoxetic Acid-enhanced MR Imaging and Dynamic CT. Radiology. 2016 Oct 31:160639. [Epub ahead of print].
[3]Tsunematsu S, Chuma M, Kamiyama T, et al. Intratumoral artery on contrast-enhanced computed tomography imaging: differentiating intrahepatic cholangiocarcinoma from poorly differentiated hepatocellular carcinoma. Abdom Imaging. 2015;40(6):1492-1499.
[4]Li Z, Bonekamp S, Halappa VG, et al. Islet cell liver metastases: assessment of volumetric early response with functional MR imaging after transarterial chemoembolization. Radiology. 2012;264(1):97-109.
[5]Suo S, Zhang K, Cao M, et al. Characterization of breast masses as benign or malignant at 3.0T MRI with whole-lesion histogram analysis of the apparent diffusion coefficient. J Magn Reson Imaging. 2016;43(4):894-902.
Figures