2084
Noninvasive Quantification of Prostate Cancer Using IVIM:evaluation of IVIM perfusion-related parameters by comparing to quantitative DCE-MRI1Tianjin First Center Hospital, tianjin, People's Republic of China, 2Philips Healthcare, Beijing, People's Republic of China
Synopsis
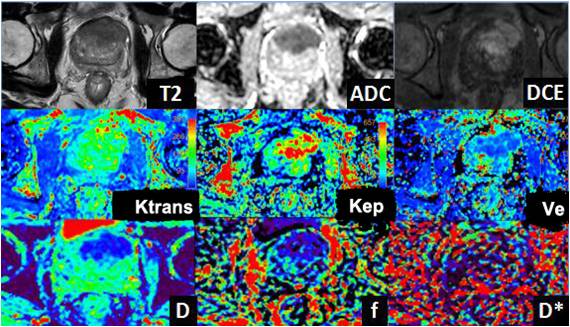
The purpose of the study was to evaluate the clinical usefulness of IVIM technique for the PCa and furtherly investigate the diffusion and perfusion characteristics among PCa, normal peripheral zone (PZ) and central gland (CG) comparing to pharmacokinetic parameters based on quantitative DCE-MRI. The IVIM was performed at 11 b values of 0, 10, 20, 30, 50, 75, 100, 250, 500, 750 and 1000s/mm2. The
D value in prostate cancer were significantly lower than those
in the PZ and CG. The perfusion fractions in PCa were significantly higher than those in the PZ. There were no significant differences in the PCa, PZ and CG for the D*, which had large SDs. D showed significant negative correlations with Ktrans and Kep respectively, while f showed a significantly positive correlations with Ktrans and Kep. IVIM can provide more detailed information on perfusion and diffusion of prostate cancer noninvasively without intravenous contrast agent administration.
Purpose
Methods
The local institutional review board approved this study. Twenty patients with prostate cancer and 17subjects with no prostate cancer (mean 71±6years; 50 Pca areas, 34 PZ, 34 CG) with TRUS biopsy or prostatectomy after MR examination were recruited in this study. The data acquisitionwas performed by using a 3.0T MRI scanner (Ingenia, Philips Healthcare, Best, the Netherlands) with 16-channel torso coil. The sequences included axial and coronal T2WI, axial IVIM and DCE-MRI. The IVIM protocol was performed with TR/TE=6000/54ms,slice thickness=3mm, FOV=240×240mm,matrix size=96×96, slices=22. The diffusion weighting was performed along three orthogonal directions with 11 b values of 0, 10, 20, 30, 50, 75, 100, 250, 500, 750 and 1000s/mm2. The parameters of DCE imaging were as the following: TR/TE=4/2ms,flip angle=12 degree, slice thickness=3mm, FOV=240×240mm.
Regions of interest (ROIs) were placed within proven PCa, normal PZ and CG
by referencing histopathological results to calculate the parameters of IVIM
and quantitative DCE-MRI. Data were fitted with IVIM bi-exponential model by
using DWI post-processing software performed in a proprietary programming
environment (PRIDE; Philips Medical Systems). Bi-exponential function analysis
was performed to derive the diffusion coefficients (D), perfusion fractions (f)
and the perfusion-related diffusion coefficient (D*). Quantitative DCE
parameters, including the volume transfer constant (Ktrans), the fractional
volume of extravascular extracellularspace (Ve) , and the rate constant of each
extraocular muscles (Kep), were analyzed. Each diffusion and perfusion
parameter for PCa, PZ and CG was compared by analysis of variance (ANOVA) using
IBM SPSS Statistics 20.0 (Armonk, New York, USA). And P<0.05 indicated a
significant difference. The Ktrans,Ve, Kep calculated with quantitative DCE-MRI
were compared to diffusion parameters (D, f, D*) using the Pearson correlation
(for normal distribution data) and Spearman's correlation(for non-normal
distribution data).
Results
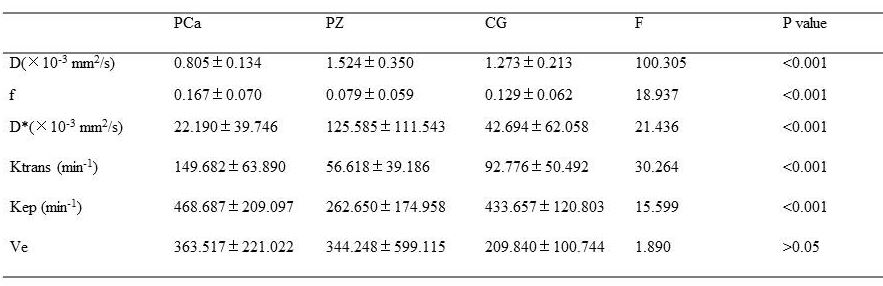
The diffusion coefficient (D) in prostate cancer were significantly lower than those in the PZ and CG (P <0.05), and D in the PZ is the highest. The perfusion fractions in PCa were significantly higher than those in the PZ and CG (P <0.05). There were no significant differences in the PCa, PZ and CG for the D*, which had large SDs.There are statistical differences of dynamic enhancement parameters (Ktrans and Kep) among the PCa, PZ and CG. No statistical differences were found for Ve. Ktrans and Kep values of prostate cancer were significantly higher than those in the PZ and CG (P < 0.05). But there were no statistical differences for Kep between the PCa and CG (P=0.318). D showed significant negative correlations with Ktrans and Kep respectively, while f showed significantly positive correlations with Ktrans and Kep. And f also showed a positive correlation with Ve.Conclusion
Parameters of bi-exponential analysis of IVIM showed significant correlations with Ktrans and Kep. They can provide more detailed information on perfusion and diffusion of prostate cancer noninvasively without intravenous contrast agent administration. And IVIM makes it possible to assist in the diagnosis of prostate cancer in the central gland. It might be very helpful in the diagnosis and monitoring therapy efficacy of prostate cancer.Acknowledgements
No acknowledgement found.References
1. Le Bihan D, Breton E, Lallemand D, et al. Radiology 1988; 168:497–505
2. Shinmoto H et al, Magn Reson Imaging 2009: 27: 355-359.
3. Mazaheri Y, Vargas HA, Akin O, et al. J Magn Reson Imaging. 2012;35(3):660-668.
4. Döpfert J, Lemke A, Weidner A, et al. Magn Reson Imaging. 2011; 29(8):1053-1058.
5. Mariacristina V , Chiara Z , Davide F, et al. European Journal of Radiology. 2016;85:790-794.
Figures