2082
The Histogram analysis of quantitative Dynamic enhanced and Diffusion-weighted Intravoxel Incoherent Motion MRI for pathologic Gleason grading of prostate cancer1Department of imaging, The second affiliated hospital of Soochow university, Soochow, People's Republic of China, 2The second affilicated hospital of Soochow university, soochow, People's Republic of China, 3The second affilicated hospital of Soochow university, People's Republic of China, 4GE healthcare China
Synopsis
There are different treatments for low-risk and high-risk prostate cancer patients in clinical, NCCN guidelines recommend proactive monitoring management as the preferred treatment for patients with low risk PCa(GS ≤6 ),and active measures for intermediate/high-risk patients. Our research found that both DCE and IVIM quantitative parameters Histogram analysis results can successfully distinguish LG from HG PCa ,and their diagnostic performance was not statistically significant. Considering the method we used to acquire quantitative parameters of DCE-MRI , IVIM may provide us a new way for those who cannot bear the invasive intravenous injection of contrast agent .
Introduction
To investigate the value and diagnostic efficiency of the quantitative DCE-MRI and IVIM parameters using 3D-histogram analysis for prostate cancer grading .Methods
A total of 53 patients pathologically confirmed as prostate cancer were included in this retrospective study. All the patients were performed by DCE-MRI and DWI-sequecne. . Data were post-processed by a non commercial software(OminiKinetics, GE Healthcare, China)For data analysis, firstly, all lesions were contoured with ROI volumically (3D ROI) , images was DCE MRI quantitative analysis parameters, Ktrans, Kep ,Ve and IVIM related quantitative parameters ADC, D, f, D* of the lesions were achieved and registrated based on T2WI.Then, histogram analysis was performed on these 3D ROIs to obtain the mean, median, 25th percentile, 75th percentile,Skewness and Kurtosis of DCE-MRI and IVIM parameters. Spearman rank correlation analysis was used to evaluate the correlation of DCE-MRI and IVIM quantitative parameters and different GS score of prostate cancer. The diagnostic performance of identifing low-grade GS score (LG, GS ≤6) and intermediate/high-grade GS score(HG, GS > 6) of prostate cancer by Receiver Operating Characteristic curve (ROC curve).Results
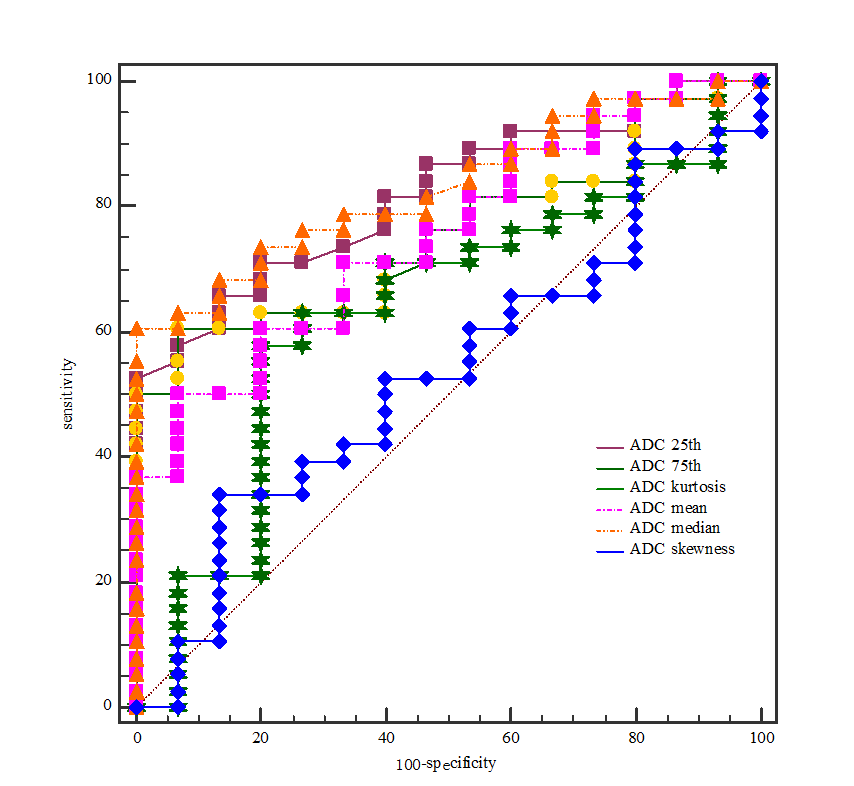
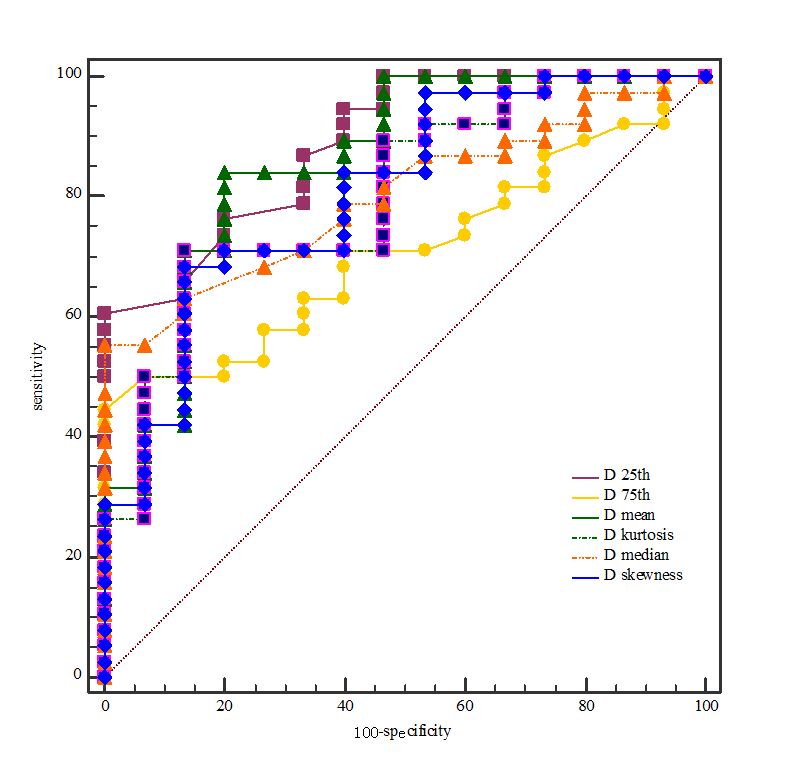
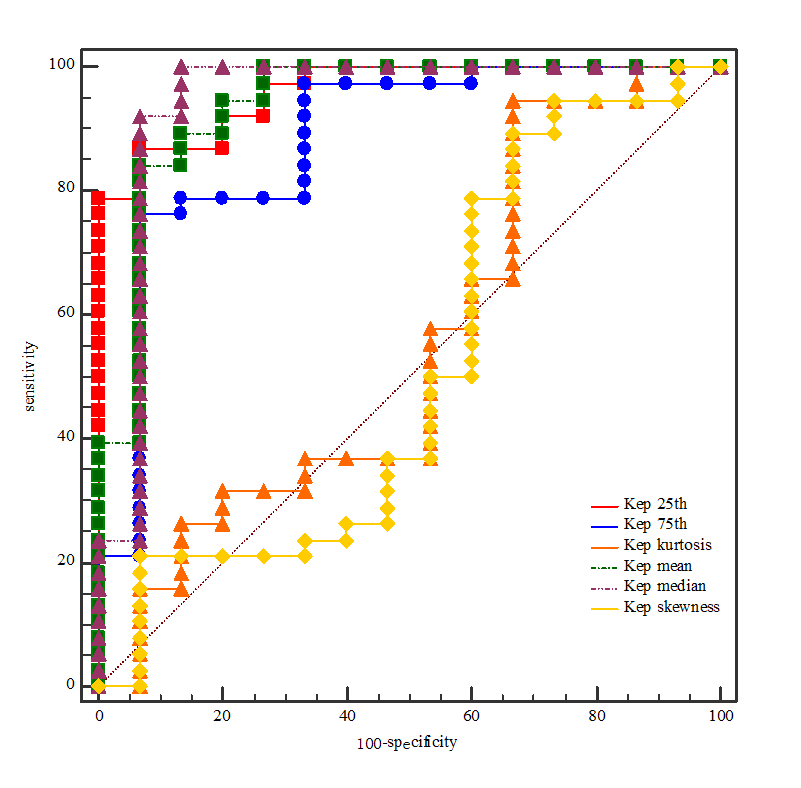
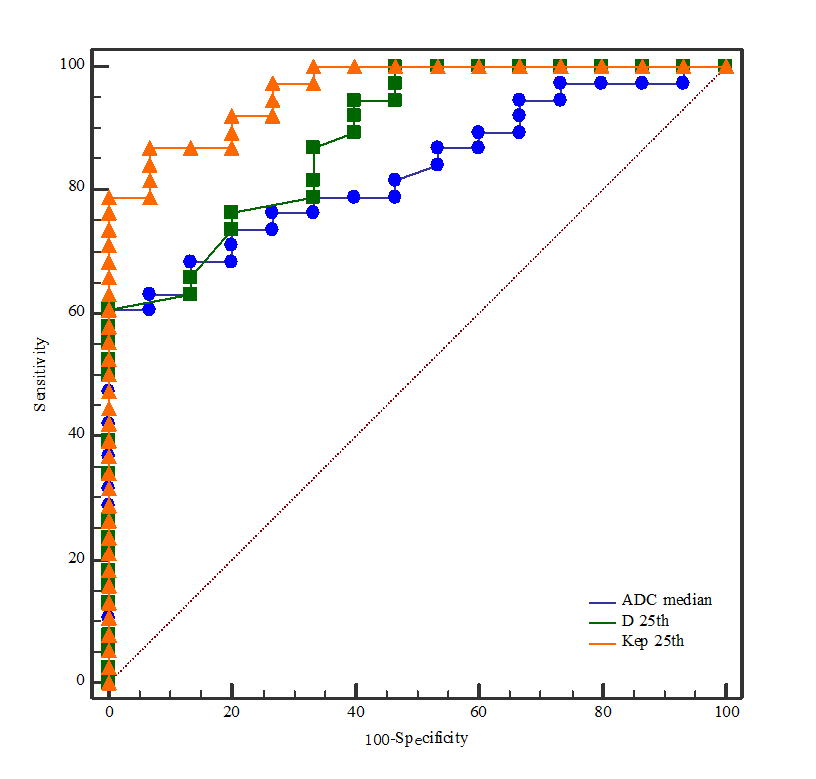
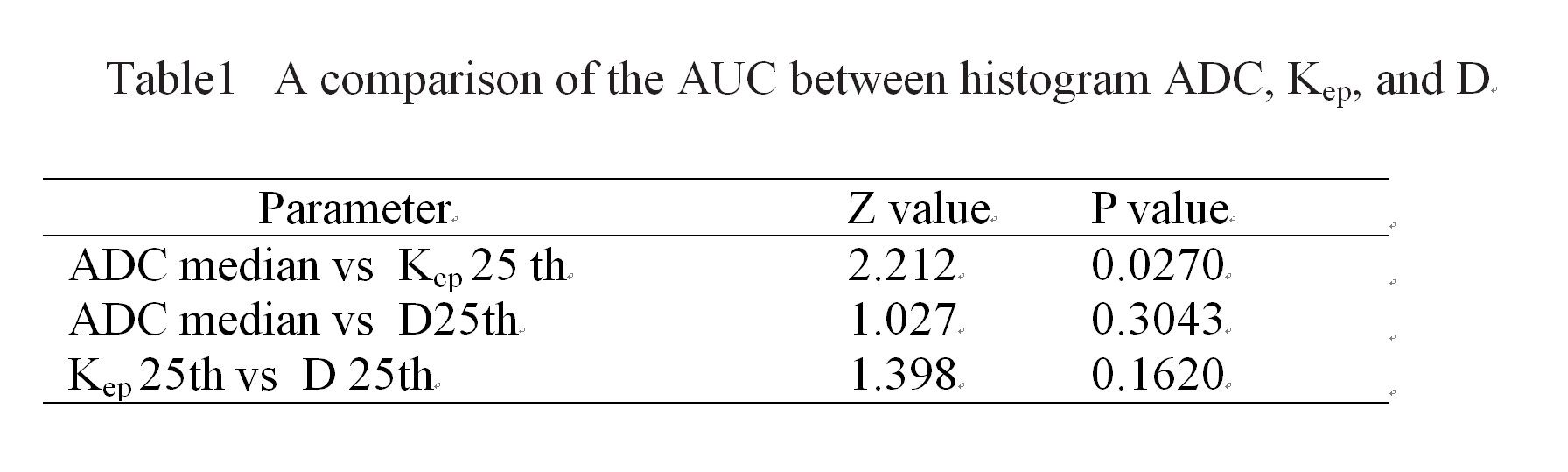
Of 53 patients with prostate cancer , GS ≤6 was 15, GS 7 was 20,GS≥8 was 17. The Ktrans and Kep and (mean, median, 25 th, 75 th) had a certain correlation with different GS score (r value was 0.346 ~0.696, P < 0.05). The ADC (mean, median, 25 th, 75 th), D (mean, median, 25 th, 75 th, Skewness, Kurtosis), D * (25 th) had a certain correlation with different GS score (r value was -0.275~-0.544, P < 0.05). The ROC analysis of DCE MRI and IVIM three-dimensional Histogram quantitative analysis parameters to identify different GS score of prostate cancer, ADC (median), D (25 th) and Kep (25 th) had higher AUC( 0.832, 0.888, 0.961).Discussion
Our resultsh showed that both and IVIM quantitative parameters 3D Histogram analysis can distinguish LG from HG PCa ,however, their diagnostic performance was not statistically significant. Compared with DCE-MRI requirements of injection of constrast media,IVIM may offer us a new way for those patients who cannot bear the invasive intravenous injection of contrast agent .Conclusion
DCE and IVIM quantitative parameters (Kep, Ktrans, ADC, D) Histogram analysis results correlated with different GS score, and can distinguish LG from HG PCa respectively. The difference of DCE and IVIM quantitative parameters Histogram analysis results to identify LG and HG of PCa was not statistically significant.Acknowledgements
The authors of this manuscript declare no relationshipswith any companies whose products or services may be related to thesubject matter of the article.References
1.Sanz-Requena R, Martí-Bonmatí L, Pérez-Martínez R, et al. Dynamic contrast-enhanced case-control analysis in 3T MRI of prostate cancer can help to characterize tumor aggressiveness[J]. European Journal of Radiology, 2016, 85(11):2119-2126.
2.Wu X, Reinikainen P, Vanhanen A, et al. Correlation between apparent diffusion coefficient value on diffusion-weighted MR imaging and Gleason score in prostate cancer.[J]. Diagnostic & Interventional Imaging, 2016.
3.Oto A, Yang C, Kayhan A, et al. Diffusion-weighted and dynamic contrast-enhanced MRI of prostate cancer: correlation of quantitative MR parameters with Gleason score and tumor angiogenesis.[J]. American Journal of Roentgenology, 2012, 197(6):1382-90.
4.Hötker A M, Mazaheri Y, Aras Ö, et al. Assessment of Prostate Cancer Aggressiveness by Use of the Combination of Quantitative DWI and Dynamic Contrast-Enhanced MRI.[J]. American Journal of Roentgenology, 2016:1-8.
5.Rozenberg R, Thornhill R E, Flood T A, et al. Whole-Tumor Quantitative Apparent Diffusion Coefficient Histogram and Texture Analysis to Predict Gleason Score Upgrading in Intermediate-Risk 3 + 4 = 7 Prostate Cancer.[J]. American Journal of Roentgenology, 2016, 206(4):775-782.
6.Peng Y, Jiang Y, Yang C, et al. Quantitative analysis of multiparametric prostate MR images: differentiation between prostate cancer and normal tissue and correlation with Gleason score--a computer-aided diagnosis development study[J]. Radiology, 2013, 267(3):787-96.
7.Yang D M, Kim H C, Sang W K, et al. Prostate cancer: correlation of intravoxel incoherent motion MR parameters with Gleason score[J]. Clinical Imaging, 2016, 40(3):445-450.
8.Zhang Y D, Wang Q, Wu C J, et al. The histogram analysis of diffusion-weighted intravoxel incoherent motion (IVIM) imaging for differentiating the gleason grade of prostate cancer.[J]. European Radiology, 2014, 25(4):994-1004.
Figures