2074
Variable Refocusing Flip Angle Single-Shot Fast Spin Echo Imaging of Liver Lesions: Improved Lesion Contrast and Speed1Radiology, University of California, San Francisco, San Francisco, CA, United States, 2Radiology, Stanford University School of Medicine, Stanford, CA, United States
Synopsis
Variable refocusing flip angle single-shot fast spin echo (vrfSSFSE) decreases T2-decay related blurring, allows increased K-space coverage while maintaining clinically relevant echo times, and reduces specific absorption rate. We evaluated clinical image quality and acquisition time of vrfSSFSE for imaging liver lesions in comparison with conventional SSFSE in patients undergoing 68Ga-DOTA-TOC PET on a 3T time-of-flight PET/MRI. Quantitative analysis of 53 lesions in 27 patients demonstrated higher mean CNR with vrfSSFSE (9.9 vs. 6.7, p<0.001) and 1.7-fold increase in speed compared to SSFSE. vrfSSFSE improves liver lesion contrast with shorter scan times acquired using a single 20 second breath hold.
PURPOSE
Fast spin echo imaging of the liver is limited by long acquisition times and motion artifact.1 Compared to conventional single shot fast spin echo (SSFSE, also known as HASTE), variable refocusing flip angle SSFSE (vrfSSFSE) decreases T2-decay related blurring, allows for increased K-space coverage while maintaining clinically relevant effective echo times due to T2-decay prolongation, and reduces specific absorption rate (SAR) due to the lower flip angles employed.2 We evaluated clinical image quality and acquisition time of vrfSSFSE for imaging of liver lesions in comparison with a conventional SSFSE sequence.METHODS
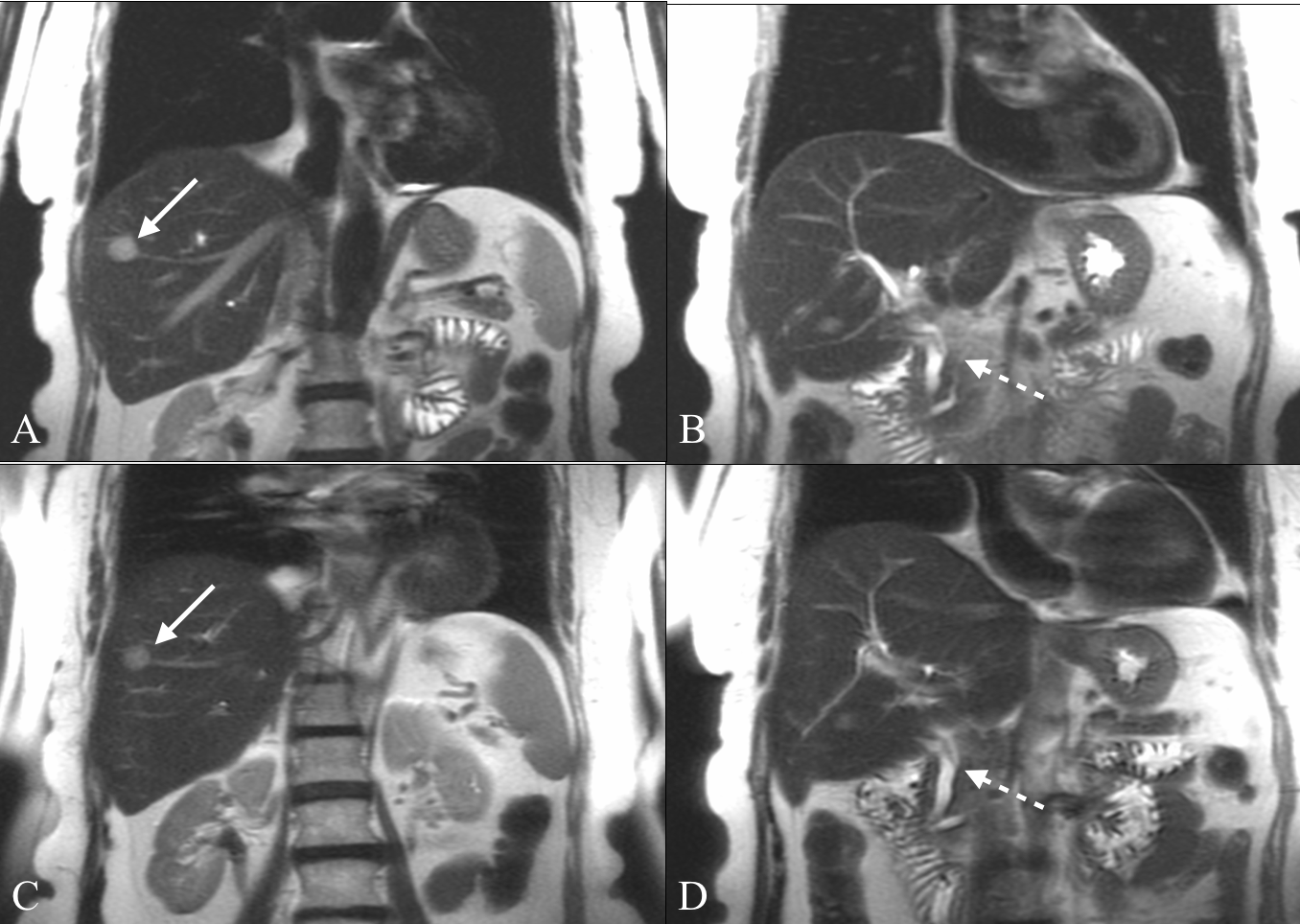
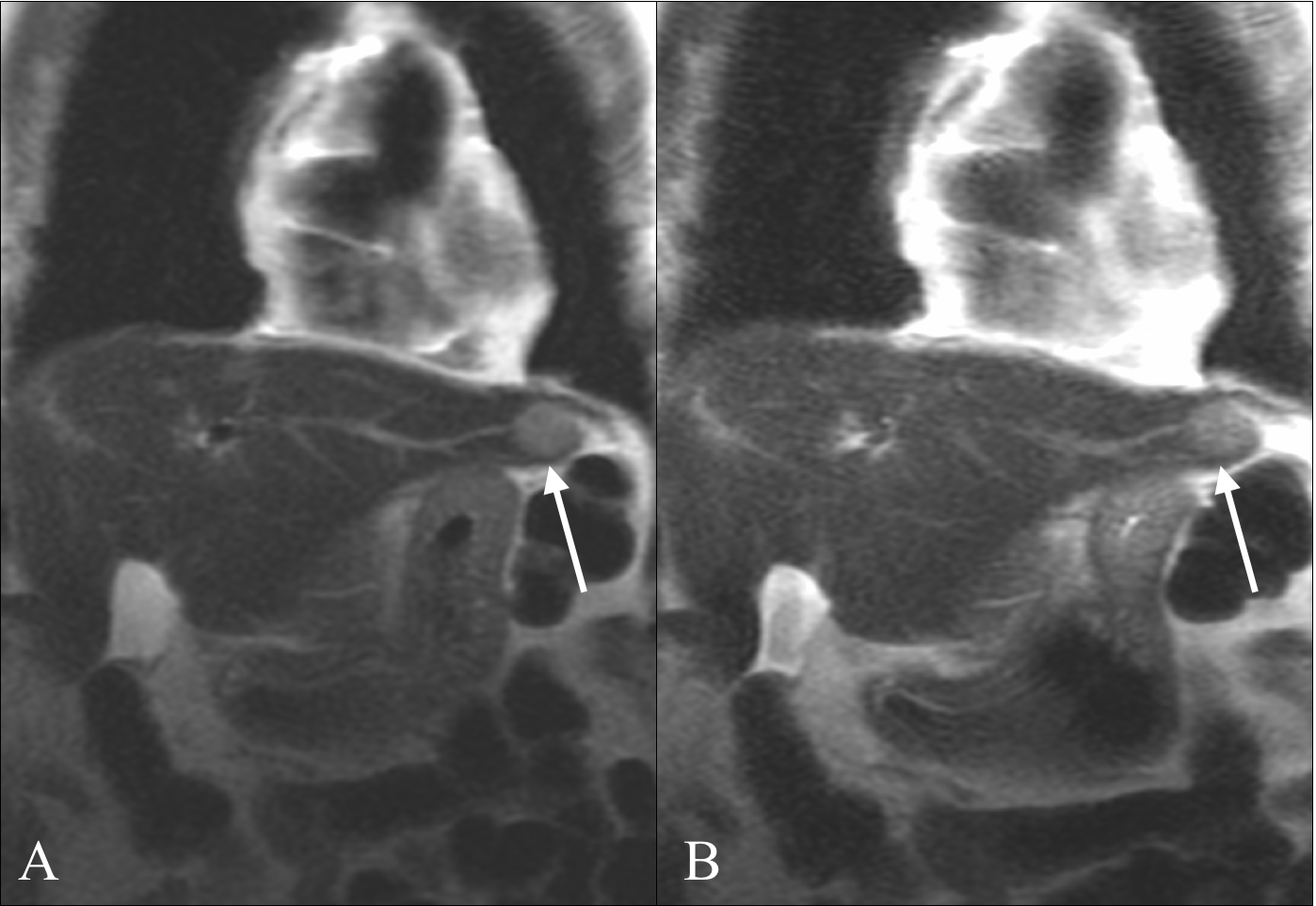
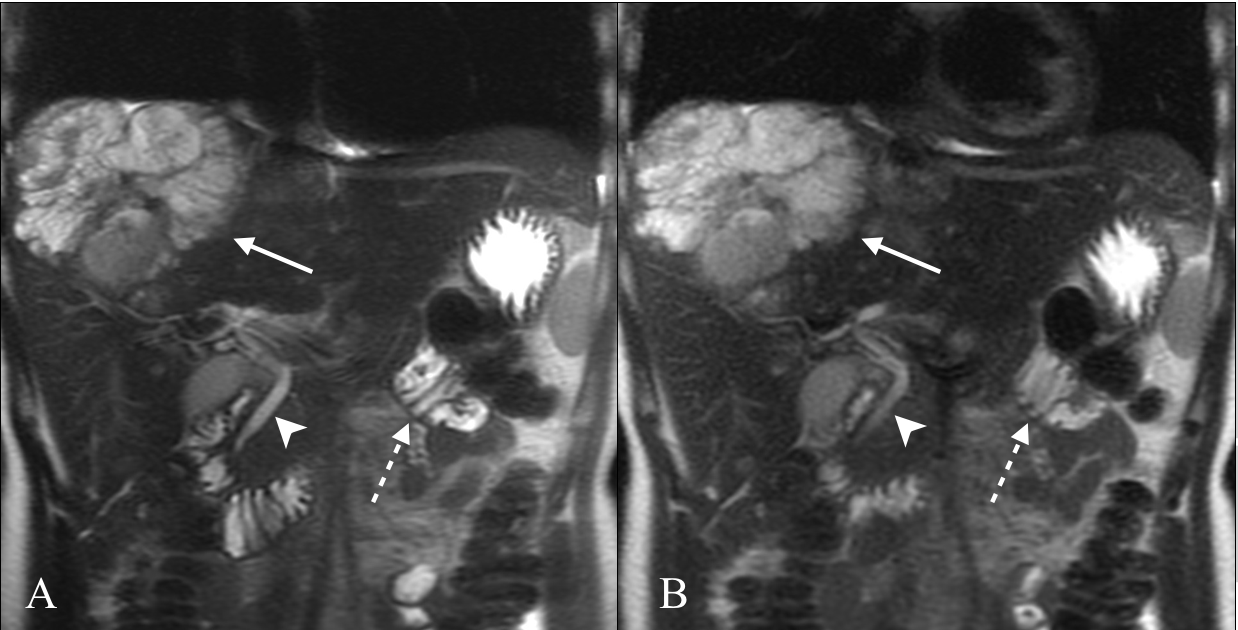
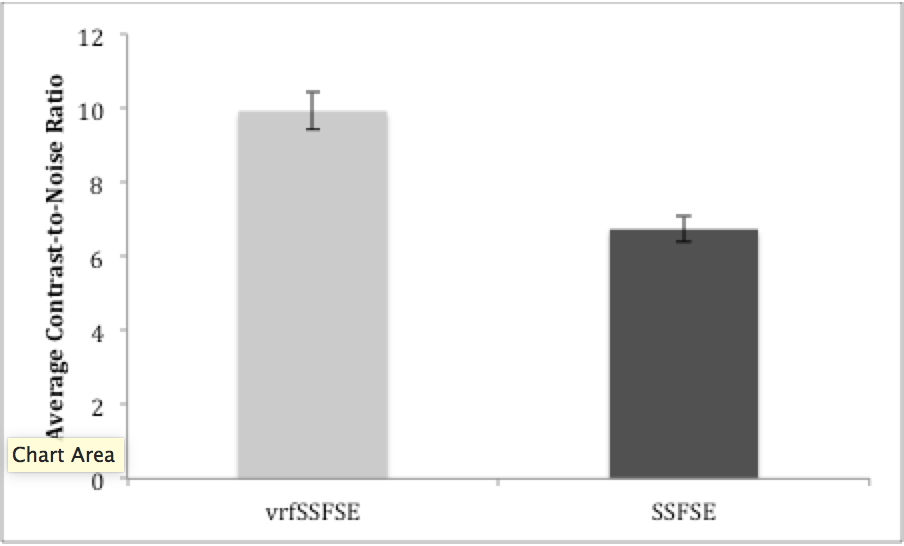
Variable refocusing flip angle SSFSE (vrfSSFSE) sequence was acquired in 46 patients with known pancreatic neuroendocrine tumors undergoing 68Ga-DOTA-TOC PET on a simultaneous time-of-flight 3.0T PET/MRI (Signa, GE Healthcare). The following imaging parameters were used for SSFSE (224 phase encodes, TE/TR of 102/1139, NEX of 54, slice thickness of 6 mm) and vrfSSFSE (224 phase encodes, TE/TR of 100/679, NEX of 71, slice thickness of 6 mm). Liver lesions ≥1.5cm with radionucleotide uptake were analyzed. Patients without metastases or metastases <1.5cm were excluded. Contrast-to-noise ratios (CNRs) were obtained using region of interest (ROI) measurements and calculated as the absolute difference in signal intensity of the lesion compared to adjacent hepatic parenchyma, divided by the standard deviation of the adjacent hepatic signal intensity. Difference in CNR was assessed using the Student’s two-tailed paired t-test with p<0.05 considered statistically significant.RESULTS
68Ga-DOTA-TOC PET/MRI identified 53 eligible lesions in 27 patients. vrfSSFSE demonstrated higher mean CNR compared to SSFSE (9.9 vs. 6.7, p<0.001). Mean repetition time (TR) was 679±97 milliseconds for the vrfSSFSE sequence compared to 1139±106 milliseconds for SSFSE, corresponding to a 1.7-fold increase in speed and 20 vs. 34 seconds to acquire a 30-slice sequence.DISCUSSION
Compared to conventional SSFSE, vrfSSFSE reduced acquisition times and improved lesion contrast on simultaneous time-of-flight 3.0T PET/MRI in patients with liver metastases. Due to the decreased SAR demands of the sequence, TR could be significantly decreased using the vrfSSFSE sequence, allowing coverage of the entire liver in a single twenty-second breath hold. This is particularly important in the setting of PET/MRI, where scan time is limited by the necessity of whole body image acquisition as well as bed specific imaging. Additionally, removing breath holds from the protocol decreases demands on the patient.CONCLUSION
Time-of-flight 3.0T PET/MRI utilizing vrfSSFSE improves liver lesion contrast and achieves shorter scan times compared to conventional SSFSE.Acknowledgements
No acknowledgement found.References
1. Yang RK, Roth CG, Ward RJ, deJesus JO, Mitchell DG. Optimizing abdominal MR imaging: approaches to common problems. Radiographics 2010;30:185-99.
2. Loening AM, Saranathan M, Ruangwattanapaisarn N, Litwiller DV, Shimakawa A, Vasanawala SS. Increased speed and image quality in single-shot fast spin echo imaging via variable refocusing flip angles. J Magn Reson Imaging 2015;42:1747-58.
3. Mannelli L, Wilson GJ, Dubinsky TJ, et al. Assessment of the liver strain among cirrhotic and normal livers using tagged MRI. J Magn Reson Imaging 2012;36:1490-5.
Figures