2069
Impact of an additional endorectal imaging coil on MR image quality and cancer detection in the prostate1Diagnostic and Interventional Radiology, Leipzig University Hospital, Leipzig, Germany, 2Institute of Pathology, University of Leipzig, Leipzig, Germany, 3Urology Department, Leipzig University Hospital, Leipzig, Germany
Synopsis
Multiparametric MRI has been shown to improve detection, localization and characterization of patients with suspected prostate cancer (PCa). The current PIRADS guideline (v2, 2015) states that the additional use of an endorectal imaging coil (ERC) increases SNR at any magnetic field strength which may be particularly useful for staging and inherently lower SNR sequences (DWI or DCE). On the other hand, phased array coils with 16 or more elements may also provide adequate SNR. This work assesses the potential benefit of an ERC for the detection of prostate cancer– within the same patients.
Purpose
Multiparametric MRI (mpMRI) has been shown to improve detection, localization and characterization in patients with suspected prostate cancer (PCa). The current PIRADS (prostate imaging reporting and data system) guideline (v2, 2015) states that the additional use of an endorectal imaging coil (ERC) increases SNR in the prostate at any magnetic field strength which may be particularly valuable for high spatial resolution imaging used in cancer staging and for inherently lower SNR sequences, such as DWI and high temporal resolution DCE [1]. On the other hand, the mere use of phased array coils with a relatively high number of elements (e.g., 16+) may also provide adequate SNR in many patients. The goal of this work was to assess, within the same patients, the potential benefit of an ERC for MRI detection of prostate cancer.Materials and Methods
Our prospective, cross-sectional study was approved by the institutional review board. Prior to radical prostatectomy, 41 male patients underwent 3T MRI. T2- and diffusion-weighted images were acquired twice using (i) surface coils combined with an endorectal coil and (ii) surface (phased-array) coils only. Two blinded readers (A and B with 70 and 160 prostate readings, respectively) randomly evaluated all image data in two separate sessions. The quality of localization- and staging-specific image features was rated on a five-point scale and cancer-suspicious lesions were assumed for PIRADS scores of 4 or 5. The standard of reference was provided by histological work-up of whole-mount sections by a senior pathologist.Results and Discussion
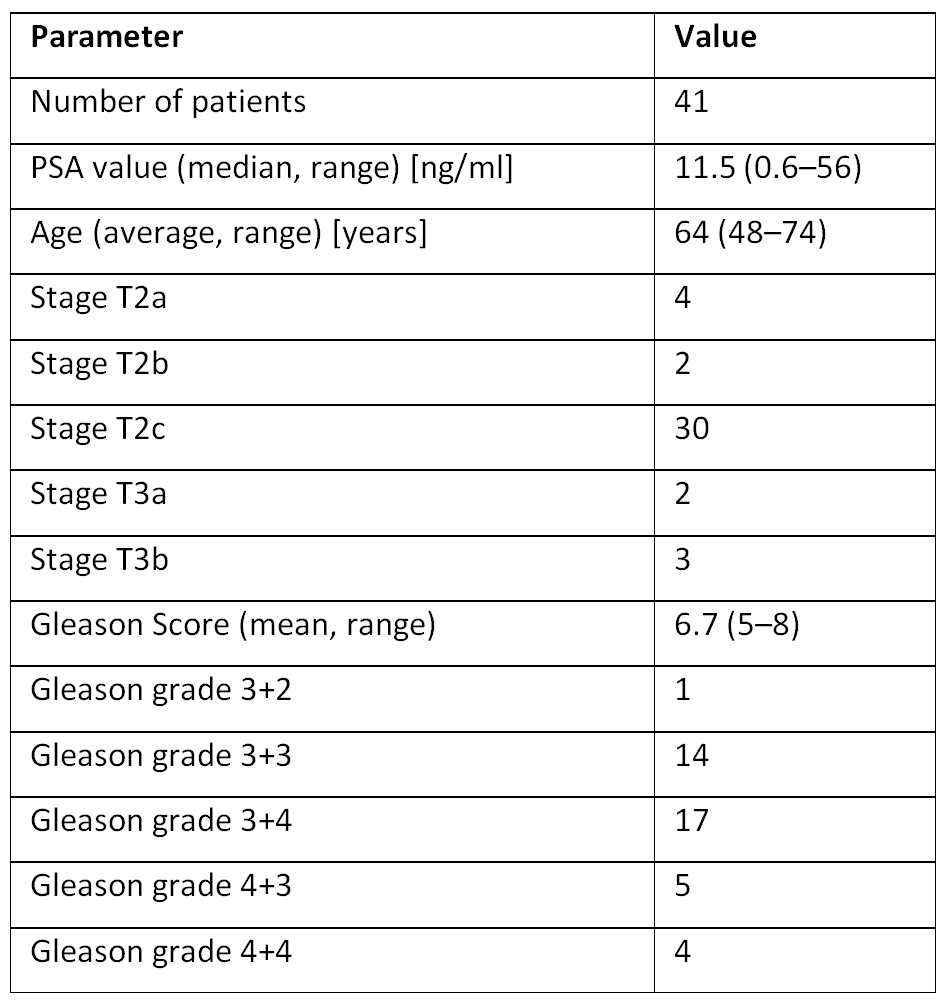
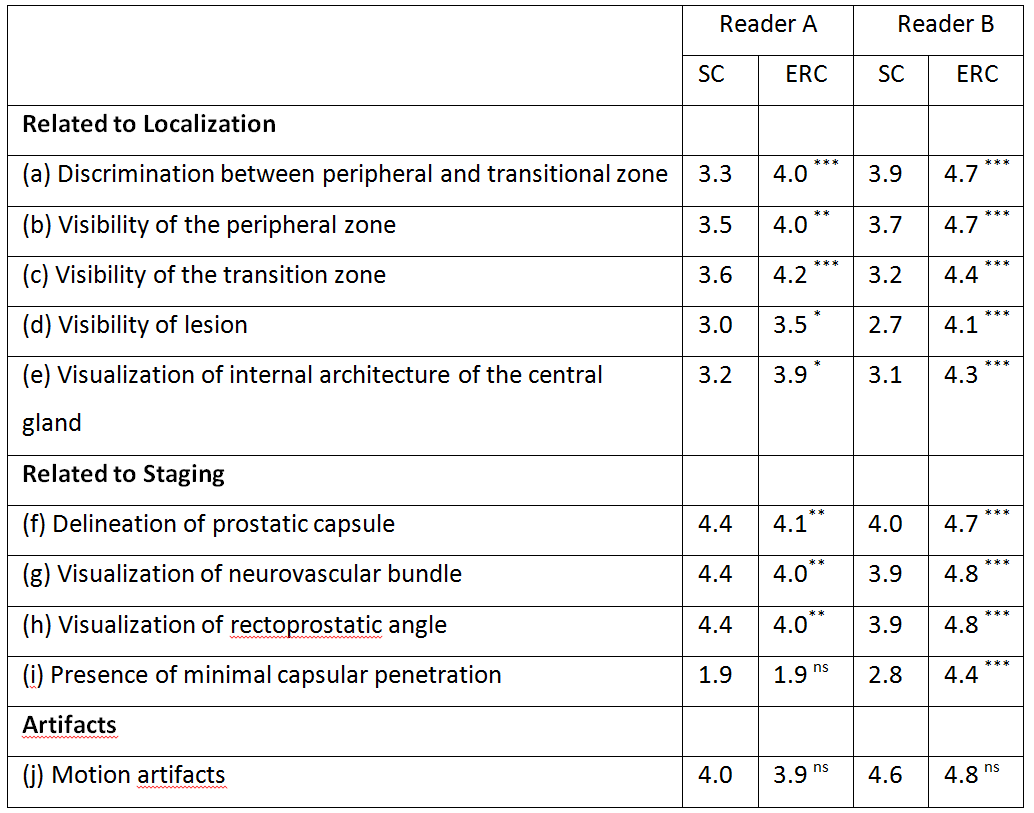
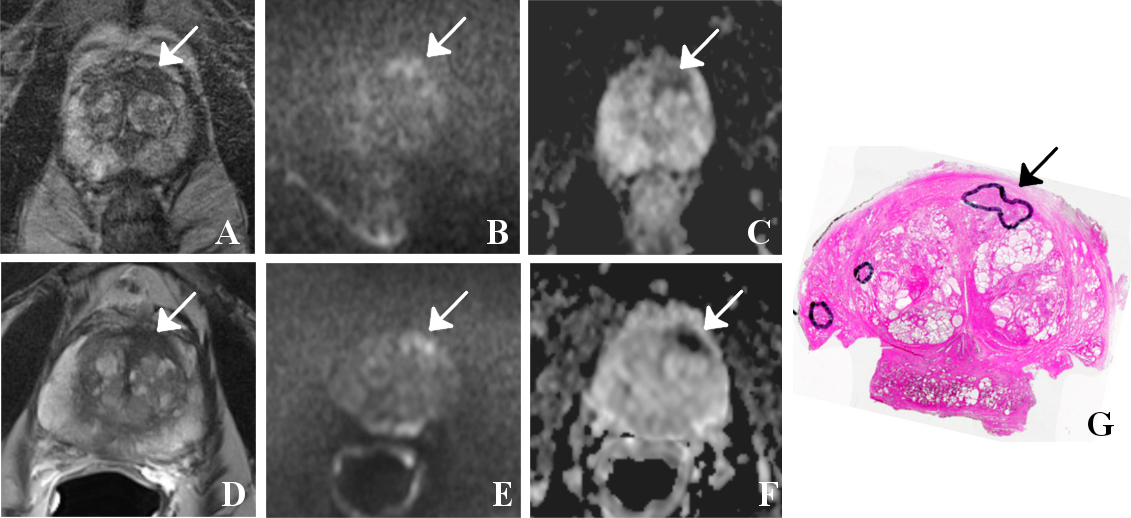
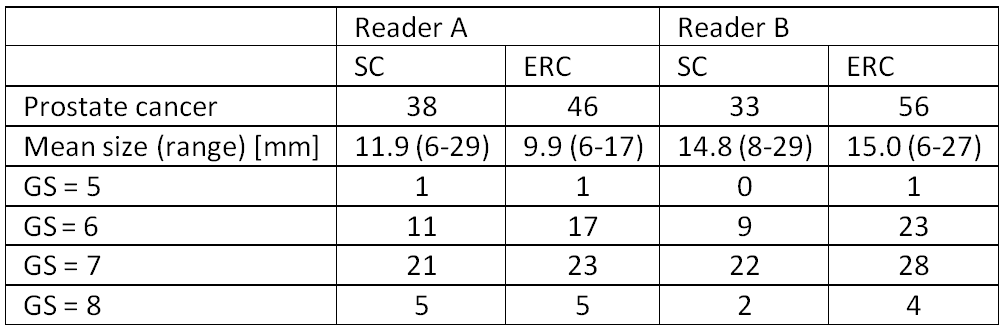
A summary of patient characteristics and histopathological results is given in Figure 1. The following results are reported as values obtained with combined coils (ERC) versus those observed with SC only. Overall, subjective scores of image quality were significantly (p<0.001) higher for ERC. A breakdown of the results for individual evaluation criteria is given in Fig. 2. Both readers reported more cancer-suspicious lesions (A: 62 vs. 49, B: 65 vs. 48). Detection rates of confirmed cancerous lesions were similar for A, 74% vs.78% (46/62 vs. 38/49), and significantly (p<0.05) higher for B, 86% vs. 69% (56/65 vs. 33/48). Both readers correctly diagnosed a higher proportion of patients with prostate cancer (A: 88% vs. 78%, B: 98% vs. 68%). Figure 3 shows a sample case of a 71 year-old patient with prostate cancer in the left transitional and peripheral zone. Figure 4 summarizes the detected PCa lesions with corresponding sizes and Gleason scores.
Conclusion
The subjectively rated 3-T MR image quality scores related to the detection, localization and staging of prostate cancer were improved with a dedicated organ coil. In terms of diagnostic performance, the numbers of true cancer foci and of patients with cancer were higher but also that of false positive results.Acknowledgements
Grant support through BMBF 13N10360 (2009-2013) is greatly acknowledged.References
[1] PIRADS v2: http://www.acr.org/~/media/ACR/Documents/PDF/QualitySafety/Resources/PIRADS/PIRADS%20V2.pdf (accessed on 11/08/2016)Figures