2063
Coronal View Renal Perfusion FAIR-ASL Measurements in Mice1Department of Physics, University of Würzburg, Würzburg, Germany, 2Department of Internal Medicine I, Division of Cardiology, University Hospital Würzburg
Synopsis
Renal perfusion measurements in coronal view using FAIR-ASL can be problematic in small animals as the selective inversion slice can label a large fraction of the inflowing blood. In this work, an alternative orientation for the selective inversion slice is shown to increase the sensitivity of the measurement.
Introduction
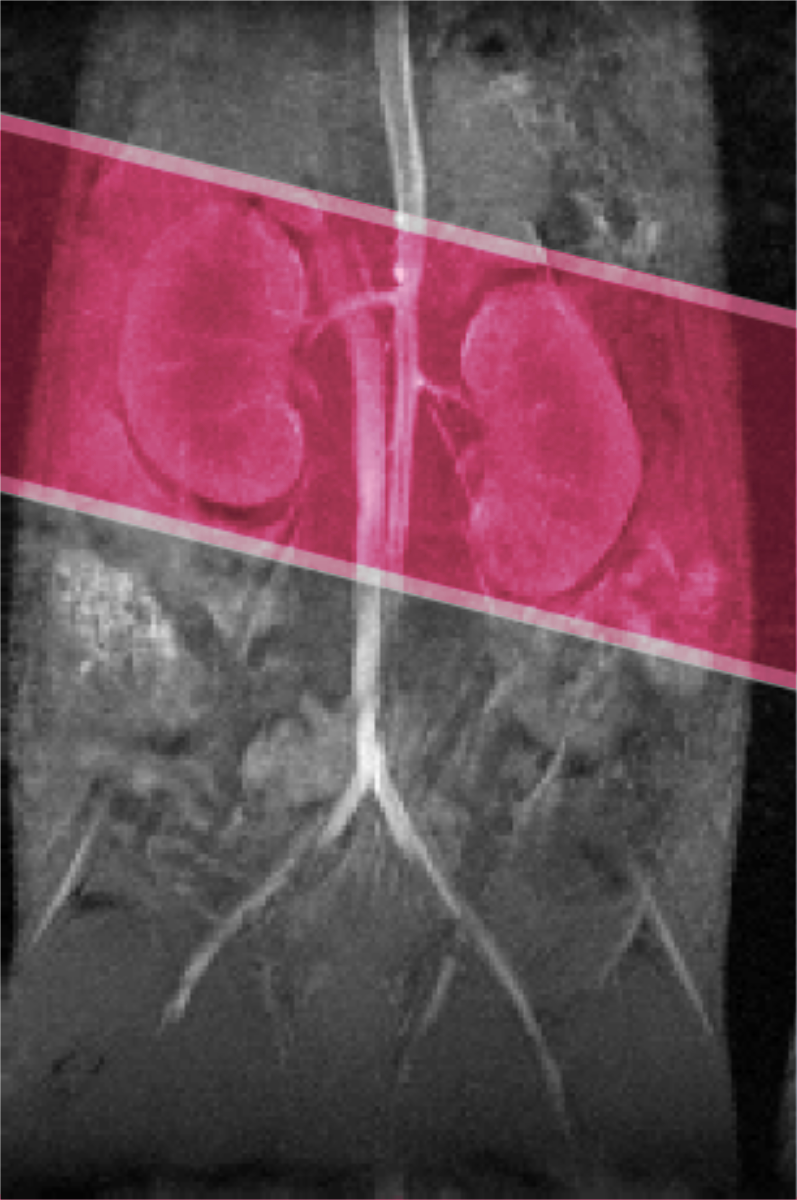
Renal perfusion is directly linked to the filtration which is one of the main functions of the kidney. MRI based kidney perfusion measurements have been used to diagnose acute kidney injury, healing processes and to provide an early indicator for transplant rejection. For these reasons quantitative kidney perfusion measurements are highly desirable. One method for the estimation of kidney perfusion used in small animals is flow sensitive alternating inversion recovery arterial spin labeling (FAIR-ASL). In FAIR-ASL, a measurement with a non-selective inversion pulse is compared to a measurement with a slice selective inversion pulse. The selective inversion slice is in the same plane as the imaging slice. It has been noted before that this is highly problematic in coronal view, as the selective slice will label inflowing blood and therefore reduce the difference between the selective and non-selective experiment[1]. This leads to low SNR and underestimation of perfusion. This problem is visualized in Fig.1. We propose to adapt the orientation of the inversion slice in the control experiment to circumvent this problem.Material and Methods
All measurements are carried out on a horizontal bore 7 T small animal system using a custom built 35 mm quadrature birdcage. A retrospectively triggered Look Locker inversion recovery method is used in combination with a model based reconstruction[2]. The standard FAIR approach is compared to the modified measurement in which the selective inversion slice is set perpendicular to the imaging plane. The inversion slice thickness is modified and rotated to extend both kidneys by 1 mm on both sides (see red marker in Fig. 1) A T1* based quantification method is used in order to acurately reconstruct perfusion values close to the edge of the slice[3].Results
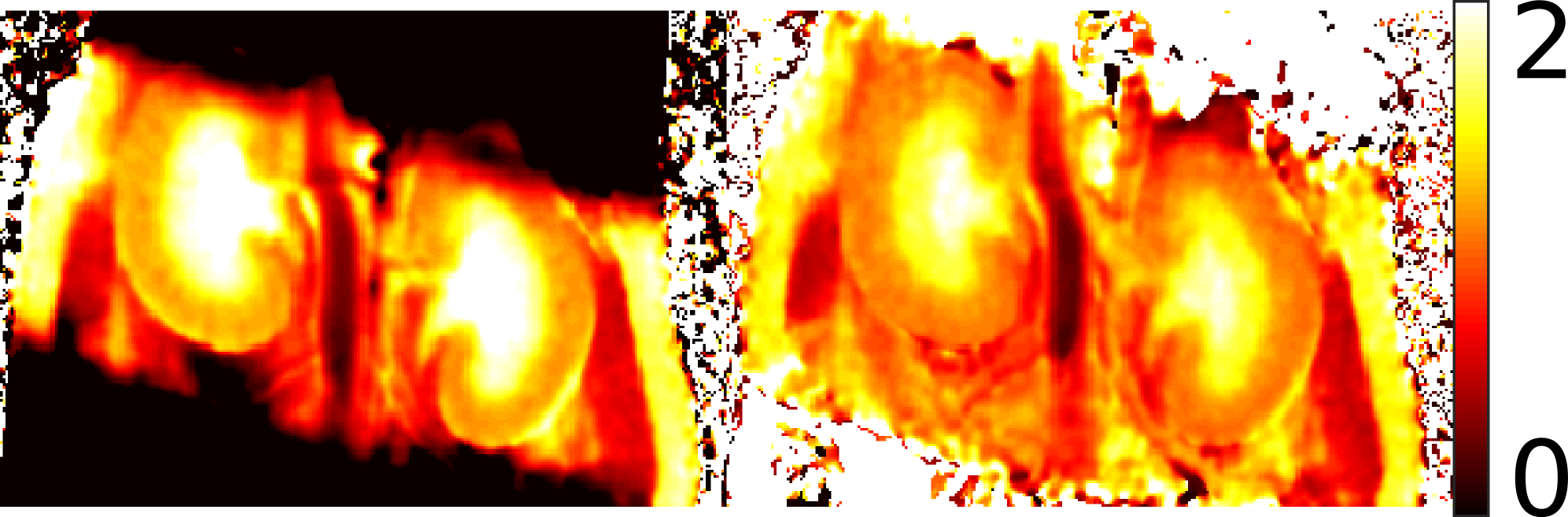
In Fig. 2, a T1 and the corresponding T1* map reconstructed from the the selective inversion slice experiment are shown. It can be seen that the T1 map underestimates T1 on the edges of the inversion slice. This would lead to strong overestimation of perfusion in these areas using the standard perfusion quantification for T1 based FAIR-ASL. A modified quantification method proposed in [3] uses the T1* map which is stable over the area containing the whole kidney enabling consistent reconstruction of renal perfusion values.
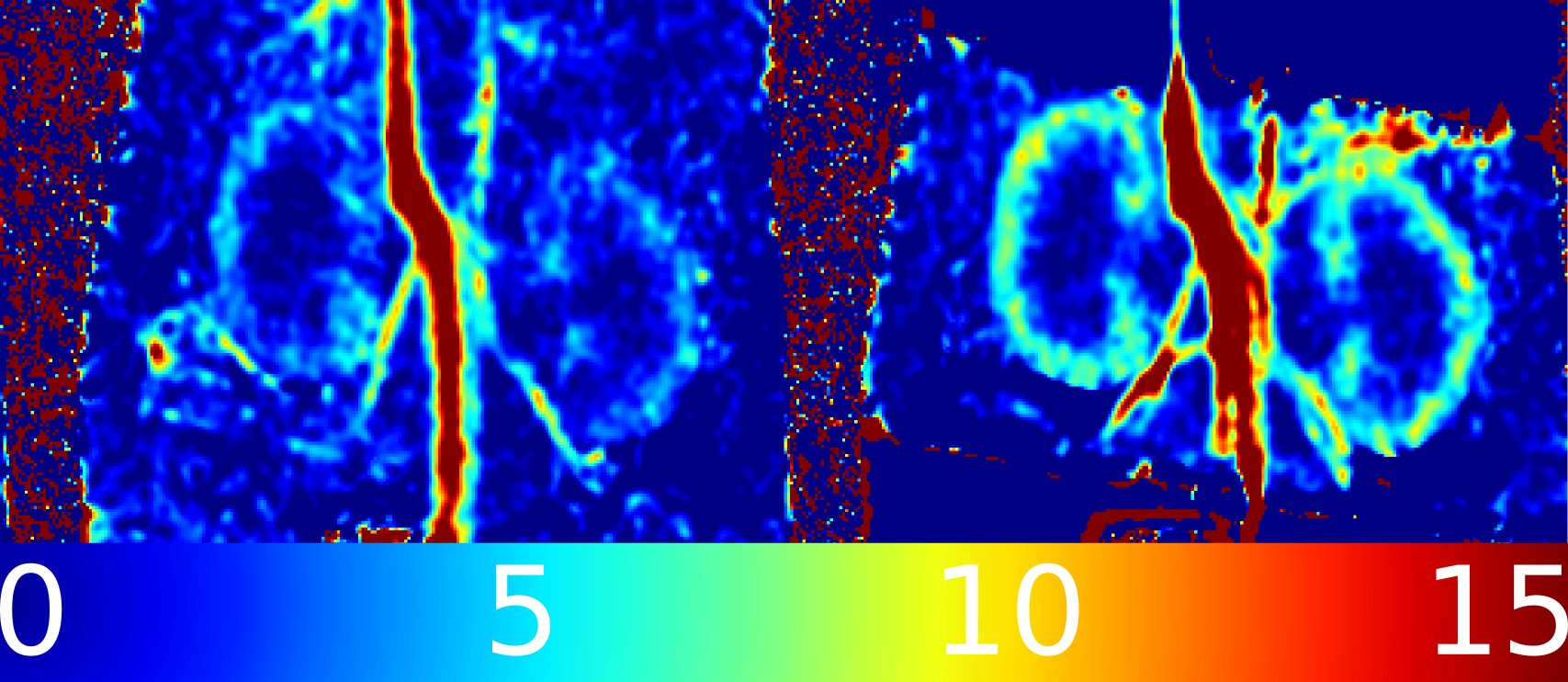
Perfusion maps acquired using the perpendicular orientation of the selective inversion slice show over 30 % higher perfusion values.
In Fig. 3, exemplary perfusion maps acquired using both schemes are compared.
Conclusion
Adjusting the position of the selective inversion slice is of great importance to the quality of the measurement. By adjusting the amount of unwanted labeled inflowing blood, the sensitivity was increased by over 30% in comparison to the standard FAIR-ASL approach.Acknowledgements
This work was supported by grants from the Deutsche Forschungsgemeinschaft (SFB 688 B5, Z02) and the Bundesministerium für Bildung und Forschung(BMBF01 EO1004)References
[1] Cutajar M, et al. Magn Reson Materials in Physics, Biology and Medicine 2012;25(2):145–153
[2] Gutjahr FT, et al. Magn Reson Med 2015;74(6):1705–1715
[3] Kampf T, et al. Magn Reson Med 2014;71(5):1784–1797
Figures