2048
Quiet Motion-Robust Technique for 4D T1-Weighted Fat-Suppressed Abdominal Imaging1Global MR Applications and Workflow, GE Healthcare, Madison, WI, United States, 2Global MR Applications and Workflow, GE Healthcare, Hino, Japan, 3Global MR Applications and Workflow, GE Healthcare, Houston, TX, United States, 4Global MR Applications and Workflow, GE Healthcare, Menlo Park, CA, United States
Synopsis
Acoustic noise generated by MR systems represents one of the major barriers to patient comfort, particularly for the pediatric population. Reducing the slew rate of the gradient field is one way to effectively decrease acoustic noise; however, this comes at the expense of scan time. For breath-hold abdominal imaging, longer scan times mean a more stressful breath-hold for the patient, reduce temporal resolution for multi-phase imaging, and may allow for more motion artifact due to suboptimal breath-holding. This work describes an accelerated 3D multi-phase technique compatible with fat saturation for both quiet and motion-robust abdominal imaging.
Purpose
Dynamic contrast-enhanced (DCE) imaging of the abdomen requires a 3D multi-phase T1-weighted fat-suppressed pulse sequence, ideally with temporal resolution high enough to adequately capture the arterial phase. Given the additional needs to fit this acquisition within a reasonable breath-hold and/or minimize motion artifact which becomes more significant with prolonged scanning, the MR system’s gradient field performance specifications must be sufficiently high. With increasing maximum gradient field slew rate comes greater acoustic noise, which for some patients, particularly the pediatric population, may prohibit a successful exam.
The DISCO1 application, with fat suppression via the two-point Dixon method and temporal acceleration via optimized view segmentation/ordering/sharing, is a DCE solution; however, regulating the maximum gradient field slew rate, and thus prolonging the scan, to improve patient comfort presents two challenges. First, the two-point Dixon method still acquires fat signal, and the potentially large amount of superficial fat in the anterior abdominal wall, close to anterior surface array coil elements, is a major source of ghosting artifact in the presence of motion. Second, two-point Dixon techniques may have a restriction on echo spacing, especially at higher field. A single-echo derivative of DISCO compatible with intermittent chemical saturation may be a more robust solution for quiet imaging.
Methods
Axial 4D breath-hold abdominal images of healthy adult volunteers were acquired with IRB approval on a 3 T whole-body scanner (MR750, GE Healthcare, Waukesha, WI, USA) with maximum gradient field amplitude/slew rate per axis: 50 mT·m-1/200 T·m-1·s-1. A 32-channel body array coil (GE Healthcare, Waukesha, WI, USA) was used. A single-echo derivative of the DISCO application compatible with intermittent chemical saturation was configured with the following protocol: flip angle: 12°, TE/TR: 1.1/3.2 ms, fat saturation preparation time: 13 ms, receive bandwidth: 83.3 kHz, FOV: 42.0 × 33.6 cm, slice thickness: 4.0 cm, frequency (right-left)/phase (anterior-posterior) encodings: 320 × 192, acquired slices: 56, phases: mask plus 4, fractional echo factor: 0.83, phase partial Fourier factor: 0.70, ARC acceleration factor: 2.5, central segment size: 16%, peripheral segments: 4, actual maximum gradient slew rate limited by dB/dt for patient safety: 110 T·m-1·s-1, scan time: 12 s. Scanning was repeated using a pulse sequence designed with a maximum gradient field slew rate of 20 T·m-1·s-1, resulting in the following changes to the protocol: TE/TR: 2.2/4.9 ms, fat saturation preparation time: 15 ms, scan time: 19 s. For each scan, acoustic noise was measured from the patient microphone and at the scan room door.Results
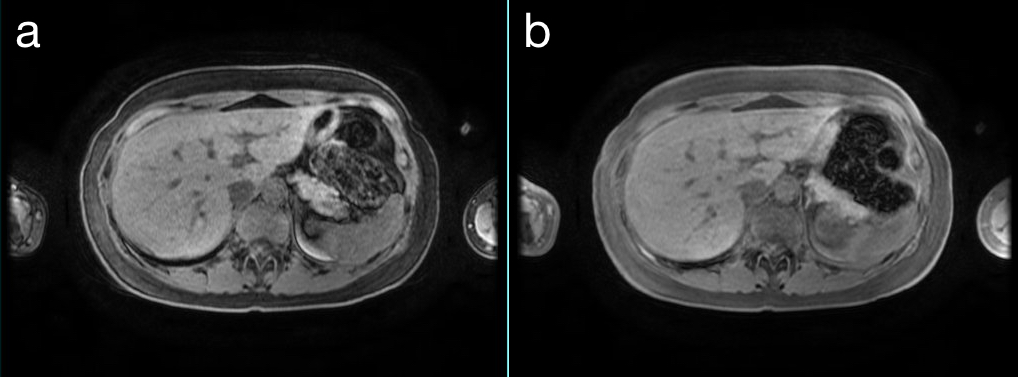
Figure 1 shows representative images at a maximum gradient slew rate of (a) 110 and (b) 20 T·m-1·s-1. Acoustic noise was measured to be 76 and 73 dB from the patient microphone and 99 and 94 dB at the scan room door for the maximum gradient slew rates of 110 and 20 T·m-1·s-1, respectively.Discussion
Qualitatively, the fat suppression technique successfully provided multiple phases with minimal motion artifact within a breath-hold of a reasonable duration. Images acquired at the reduced maximum gradient slew rate exhibited minimal additional motion artifact while perceived acoustic noise was noticeably attenuated. For certain clinical scenarios where images would be nondiagnostic without additional measures to improve patient comfort, trading off some image quality may be deemed acceptable.
Although the images shown are acquired during a breath-hold, the technique could be combined with a navigator and performed fully free-breathing in order to further improve patient comfort or handle uncooperative patients. The reduction in acoustic noise would need to be maintained during the navigator, which is possible with, for example, whole volume excitation.2 However, the lower efficiency of navigator scanning would further degrade temporal resolution. More future work could include studying the effects of contrast injection.
Conclusion
This accelerated 3D multi-phase technique compatible with fat saturation is capable of both quiet and motion-robust abdominal imaging for clinical scenarios in which success is limited by patient comfort.Acknowledgements
No acknowledgement found.References
1. Saranathan M, Rettmann DW, Hargreaves BA, Clarke SE, Vasanawala SS. Differential Subsampling with Cartesian Ordering (DISCO): a high spatio-temporal resolution Dixon imaging sequence for multiphasic contrast enhanced abdominal imaging. J Magn Reson Imaging 2012;35:1484-1492.
2. Iwadate Y, Nozaki A, Nunokawa Y, Okuda S, Jinzaki M, Kabasawa H. Silent navigator with whole volume excitation. In Proceedings of the 24th Annual Meeting of the ISMRM, Singapore, 2016. p. 1856.
Figures