2047
Using 2D-PACE to trigger scan and supervise motion on Breath-Hold imaging1Siemens Shenzhen Magnetic Resonance Ltd, Shen Zhen, People's Republic of China
Synopsis
A simple 2D pace module was implemented in a Breath-Hold imaging work flow to trigger the normal scan and supervise the motion. Our preliminary experiments show that within the newly added module, images are more immune to respiratory motion artifacts and the detail of small structures are clearer.
Purpose:
Respiratory caused motion artifact and blurring could be largely eliminated by patients breath-hold during scanning. However, artifacts were still obvious sometimes, since data acquisition started before the patient hold breath or went through different breath-hold levels on multi-breath hold situations. The problem happened especially on auto voice command scanning mode. In this work, a simple 2D PACE [1, 2] module was implemented in Breath-Hold workflow to trigger and supervise data acquisition process; volunteers experiments were performed to validate the possible improvements.
Method:
A modified 2D FLASH [Fig 1 A] sequence was designed for scout motion, flip-angle 8 degree, asymmetric echo, PE lines 16. TR 6.5ms, a scout scanning of low-resolution image took less than 70ms. The supervised region was put over the dome of liver [Fig 1 B], and the entire workflow was described on Fig 2. Scout images acquiring at voice guided study phase was used to detect the diaphragmatic peaks and troughs of motion. The process requires only one respiratory cycle, during which the trigger position was determined. The MR technologist could further define at which positions data acquisition was permitted or excluded within a certain tolerance, typically 3-6 mm. The study phase was followed by formal scanning phases, during which scout images continued supervising the dome. Once the trigger position was arrived, scout scanning stopped and imaging scanning started. Furthermore, a scout image was also acquired after image scanning, the position information difference before and after image scan reflected inter-scanning motion , an experienced tolerance was set to trigger a re-scan.Result:
In-vivo studies were performed on a 1.5 Tesla (T) MAGNETOM Aera scanner(Siemens Healthcare) with volunteers admitted for abdomen examination, an 18-channel body matrix coil was used, and 3 volunteers were tested with hasteT2 Multi-Breath-hold protocols (coronal and transversal) for abdomen imaging. The protocol parameters were follows. (1)For Haste coronal imaging: FOV = 400x400mm, TE/TR = 91/1180ms, BW/pixel = 700Hz, voxel = 1.6x1.6x6mm, TA = 50s, 33 slices with 20% slice gap, IPAT = 2; (2) For Haste transversal imaging: FOV 350X284mm, TE/TR=94/1320ms, WE/ pixel =710Hz, Voxel=1.1x1.1x6mm, TA = 49s, 30 slices with 20% slice gap. Obvious image quaulity improvements were detected on 2 cases of coronal imaging experiments[Fig 3, a-bi-d-e],
which demonstrated that navigated breath hold scannings were more immune to respiratory related artifacts [Fig 3-d] and of same data acquisition efficiency as standard Breath hold method. in addition, the detail information of small structures much clearer [Fig3-e].
Discussion:
A novel image-based self-navigation approach was implemented on conventional Breath-Hold scanning workflow. our preliminarily experiments show abvious benefits for respiratory artifacts mitigation. In addition,the conventional Breath-hold mode (auto-voice command) didn’t consider that patients might not follow the voice command very well, while adding a supervision module could make the scanning less effected by motion and get more reliable image qualities.Acknowledgements
No acknowledgement found.References
[1] Michael V. McConnell, Vaibhav C, et, al. Prospective Adaptive Navigator Correction for Breath-Hold MR Coronary Angiography[2] Zech CJ. J Magn Reson Imaging 2004; 20: 443-450.
Figures
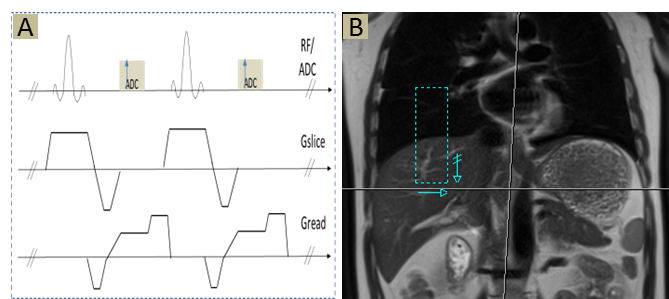
Fig 1 [A] asymmetric FLASH kernel for scout imaging; [B] pace supervise region
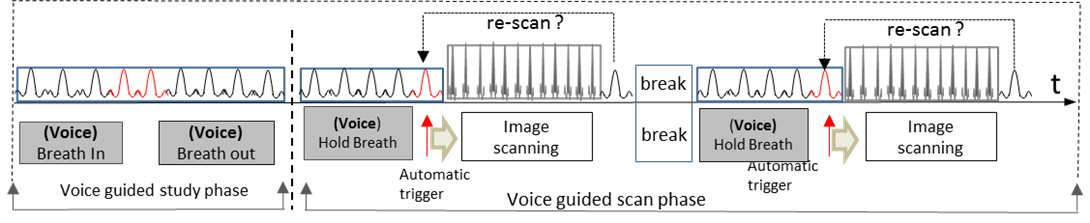
Fig 2. The work-flow of voice guide PACE in Breath-Hold imaging
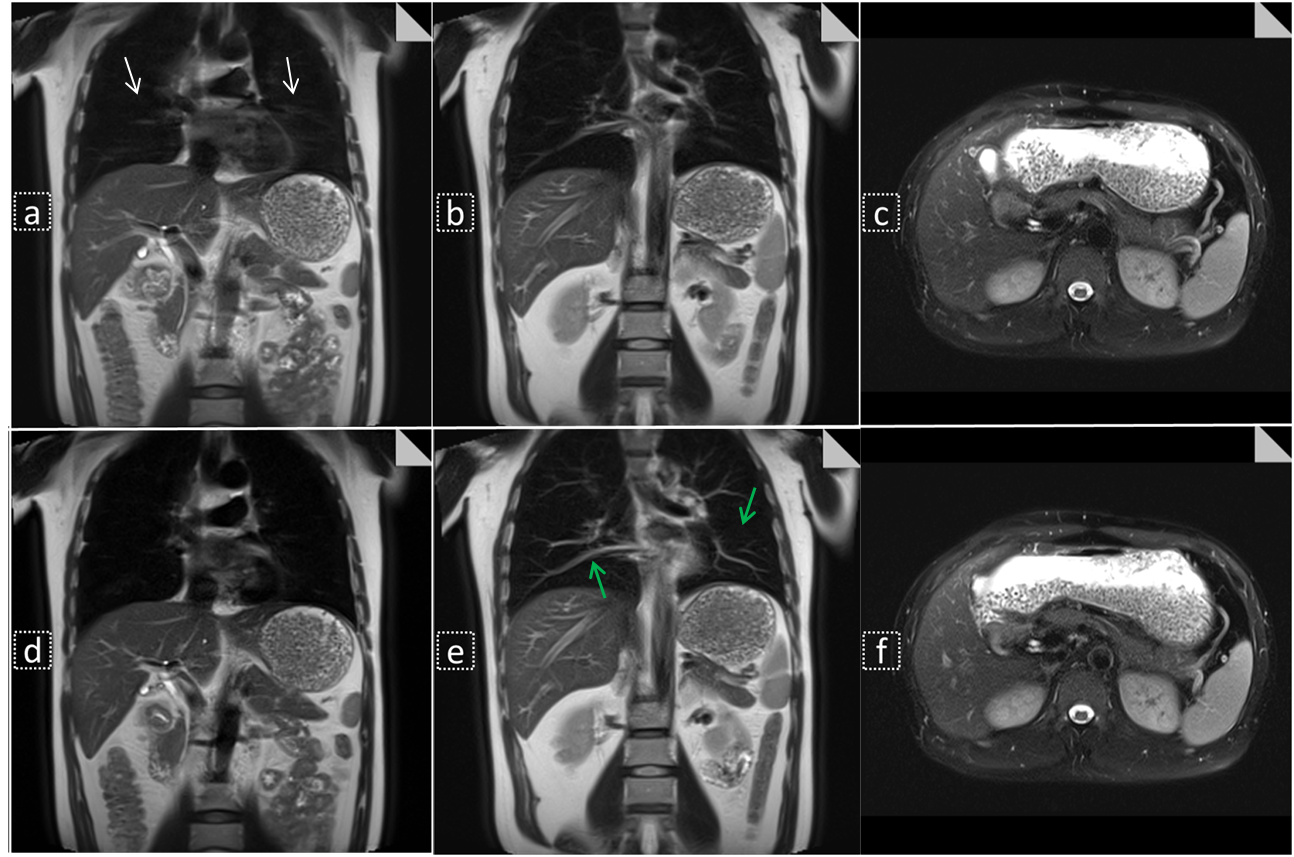
Fig 2 , compare between Breath-Hold imaging and pace-supervised Breath-Hold imaging ; [a] [b] and [c]were acquired with conventional Breath-Hold method; [d] ,[e] and [f] were acquired with pace-navigated Breath-hold method.
Motion artifacts are obviously find on [a] ( white arrow), and with pace guided Breath-Hold method, small structures or detail information was much clear and less effected by respiratory motion. There were no obvious differences on transversal images [c and f].