2043
The assessment of gallstones using three dimensional ultra-short echo time in vivo1Radiology, Seirei Mikatahara General Hospital, Hamamatsu, Japan, 2Fundamental Development for Advanced Low Invasive Diagnostic Imaging, Nagoya University, Graduate School of Medicine, 3Seirei Mikatahara General Hospital, Hamamatsu, Japan, 4Philips Electronics Japan, Ltd., Tokyo, Japan, 5Radiology, Hamamatsu University School of Medicine, Hamamatsu, Japan
Synopsis
First clinical study using 3D dual echo UTE sequence for suspected gall stone patients was performed. All gallstones were able to be detected as positive signal in-vivo. Our study may indicate that UTE has an added value of depicting impacted stones or hepatolithiasis as positive signal.
PURPOSE
Cholelithiasis is a very common disease. Gallstones can be recognized as filling defects within bright bile on the T2-weighte image. However intrahepatic stones or impacted stones in a cystic duct or a duodenal papilla can be difficult to be detected using MRCP alone for lack of high signal intensity bile surrounding the low signal intensity stones. Gallstones, especially cholesterol stones, are composed of solid-state crystal; therefore it is difficult to exploit signals on usual MRI. Recent development of ultrashort echo-time (UTE) with 3D radial sampling of the free-induction decay allows for the detection of solid object with very short T2 relaxation times such as tendons, ligaments, menisci or periosteum. 6-14 We had reported that using UTE and T1WI, all kinds of gallstones could be detected as higher CNRs than surrounding saline in vitro. It might be indicating that UTE has an added value of depicting impacted stones or hepatolithiasis. (M. Takahashi, ISMRM, 2016.05, Singapore) The purpose of this study is to test whether UTE can help depict gallstones as positive signals in-vivo.METHODS
Fourteen patients (9 male and 9 female, 41 – 77 years old ), who were suspected of having gallstone, underwent MRI including 3D dual echo UTE before the cholecystectomy. This study was approved by IRB, and all patients gave written informed consent. T1WI with fat suppression and UTE were performed. For UTE imaging, 3D radial dual-echo sequence with first echo (TE of 70 msec) (: UTE) and the second echo (2.24 msec) was perfomed. To selectively visualize only short-T2 components, subtraction images (: Subtraction) between first echo images and second echo images were processed.MR sequence parameters of UTE were as follows: dual echo of 70μsec and 2.24msec, TR 7.6msec, FA 10 degree, FOV 160 mm, 72× 72 matrix, slice thickness 2.0mm. The scan time was approximately 5min for 40 slices. Removed gallstones were visually classified as cholesterol stones or non-cholesterol stones (i.e., pigmented stones and black stones). For a semi-quantitative assessment, CNRs for gallstone to the surrounding bile were calculated on images. Statistical evaluation was performed with Dunn’s non-parametric test; p < 0.05 was considered significant.RESULTS
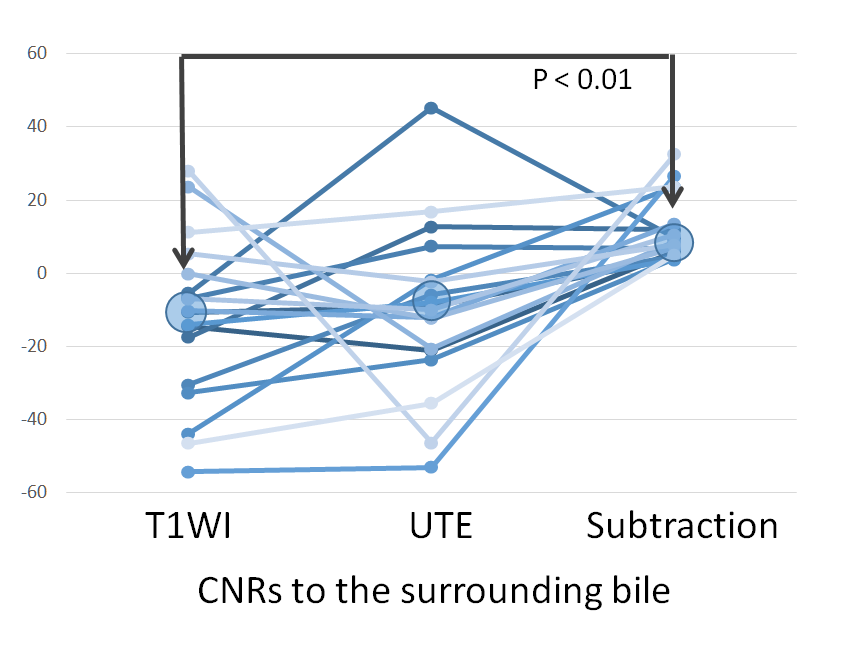
Averages (±SD) CNRs to the surrounding bile on T1WI, UTE and Subtraction imaged were -12.5 (±22.7), -9.9 (±23.0), 11.7 (±8.8), respectively. Statistically significant difference between T1WI and Subtraction image (p < 0.01) was measured. On subtraction images, all values were positive signal as compared to background bile. (Graph 1.)
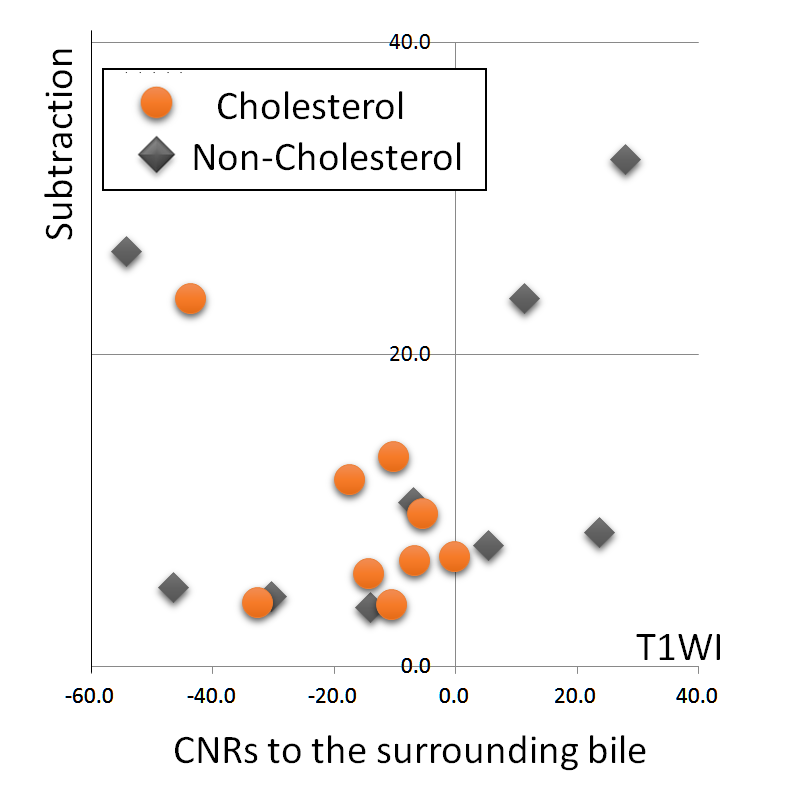
In comparison between Cholesterol and Non-Cholesterol, averages (±SD) of CNRs on T1WI were -15.7(±14.0) and -9.3 (±29.6), respectively. Likewise -1.6(±21.3) and -18.3(±22.7) on UTE, 9.7(±6.2) and 13.7(±10.9) on Subtraction. There were no statistically significant difference between two groups. On subtraction all CNRs in the both groups were positive value. On T1WI, all CNRs of Cholesterol stones were negative, but as for those of Non-Cholesterol stones, they were widely distributed from negative to positive. (Graph 2.)
DISCUSSION
In previous in-vitro study, using one of dual echo UTE and T1WI we demonstrated that all kinds of gallstones could be depicted as higher CNRs than surrounding saline signal in vitro. In this study, we tested whether UTE can help depict gallstones as positive signals compared to background bile in-vivo. The mean CNRs of gallstones on the UTE images had higher signal than those on the T1WI. Especially on subtraction images, all values were positive signal as compared to background bile. There were no significant difference between the mean CNRs of Cholesterol and Non-cholesterol stones. However if the signal on T1WI is relatively high, we can infer that the stone may be non-cholesterol. In this study we used 70 μsec for the ultra short echo time since we demonstrated that T2 values of cholesterol gallstone were distributed between 45.4 and 156μsec. (2015ISMRM) 70 μsec echo time may not be short enough. In addition, SNRs and spatial resolutions were not satisfactory. There remains a lot to be done; however, current study has implicated that UTE technique can depict all the biliary stones as positive signal, which may help depict impacted stones or intrahepatic biliary stones.CONCLUSION
By using dual echo UTE sequence, all gallstones could be detected as higher CNRs than surrounding bile, which suggested an added value of MRI in depicting impacted stone in the biliary system.Acknowledgements
No acknowledgement found.References
1: Baillie J, Paulson EK, Vitellas KM. Biliary imaging: a review. Gastroenterology. 2003 May;124(6):1686-99. Review. Erratum in: Gastroenterology. 2003 Nov;125(5):1565.
2: David V, Reinhold C, Hochman M, Chuttani R, McKee J, Waxman I, Wang L, Li W,Kaplan R, Edelman RR. Pitfalls in the interpretation of MR cholangiopancreatography. AJR Am J Roentgenol. 1998 Apr;170(4):1055-9.
3: Baillie J, Paulson EK, Vitellas KM. Biliary imaging: a review. Gastroenterology. 2003 May;124(6):1686-99.
4: Tsai HM, Lin XZ, Chen CY, Lin PW, Lin JC. MRI of gallstones with different compositions. AJR Am J Roentgenol. 2004 Jun;182(6):1513-9.
5: Ukaji M, Ebara M, Tsuchiya Y, Kato H, Fukuda H, Sugiura N, Saisho H. Diagnosis of gallstone composition in magnetic resonance imaging: in vitro analysis. Eur J Radiol. 2002 Jan;41(1):49-56.
6: Rahmer J, Börnert P, Dries SP. Assessment of anterior cruciate ligament reconstruction using 3D ultrashort echo-time MR imaging. J Magn Reson Imaging.2009 Feb;29(2):443-8.
7: Gold GE, Pauly JM, Macovski A, Herfkens RJ. MR spectroscopic imaging of collagen: tendons and knee menisci. Magn Reson Med. 1995 Nov;34(5):647-54.
8: Gatehouse PD, Bydder GM. Magnetic resonance imaging of short T2 components in tissue. Clin Radiol. 2003 Jan;58(1):1-19.
9: Reichert IL, Benjamin M, Gatehouse PD, Chappell KE, Holmes J, He T, Bydder GM.Magnetic resonance imaging of periosteum with ultrashort TE pulse sequences. J Magn Reson Imaging. 2004 Jan;19(1):99-107.
10: Glover GH, Pauly JM, Bradshaw KM. Boron-11 imaging with a three-dimensional reconstruction method. J Magn Reson Imaging. 1992 Jan-Feb;2(1):47-52.
11: Rahmer J, Börnert P, Groen J, Bos C. Three-dimensional radial ultrashort echo-time imaging with T2 adapted sampling. Magn Reson Med. 2006 May;55(5):1075-82.
12: Rasche V, Holz D, Proksa R. MR fluoroscopy using projection reconstruction multi-gradient-echo (prMGE) MRI. Magn Reson Med. 1999 Aug;42(2):324-34.
13: Yassin A, Pedrosa I, Kearney M, Genega E, Rofsky NM, Lenkinski RE. In vitro MR imaging of renal stones with an ultra-short echo time magnetic resonance imaging sequence. Acad Radiol. 2012 Dec;19(12):1566-72.
14: Du J, Corbeil J, Znamirowski R, Angle N, Peterson M, Bydder GM, Kahn AM. Direct imaging and quantification of carotid plaque calcification. Magn Reson Med. 2011 Apr;65(4):1013-20.
Figures
Graph 1.
Averages (±SD) CNRs to the surrounding bile on T1WI, UTE and Subtraction imaged were -12.5 (±22.7), -9.9 (±23.0), 11.7 (±8.8), respectively. Statistically significant difference between T1WI and Subtraction image (p < 0.01) was measured. On subtraction images, all values were positive signal as compared to background bile. (Graph 1.)
Graph 2.
In comparison between Cholesterol and Non-Cholesterol, averages (±SD) of CNRs on T1WI were -15.7(±14.0) and -9.3 (±29.6), respectively. Likewise -1.6(±21.3) and -18.3(±22.7) on UTE, 9.7(±6.2) and 13.7(±10.9) on Subtraction. There were no statistically significant difference between two groups. On subtraction, all CNRs in both groups were positive values. On T1WI, all CNRs of Cholesterol stones were negative, but as for those of Non-Cholesterol stones, they were widely distributed from negative to positive.
T1WI
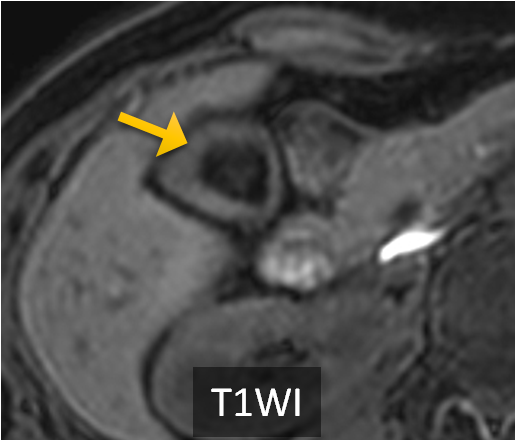
CASE 59y.o female with a cholesterol gallstone A stone could be visualized as low signal on T1WI. Even on UTE image the signal was weak, but on Subtraction image it could be clearly visualized as positive signal.
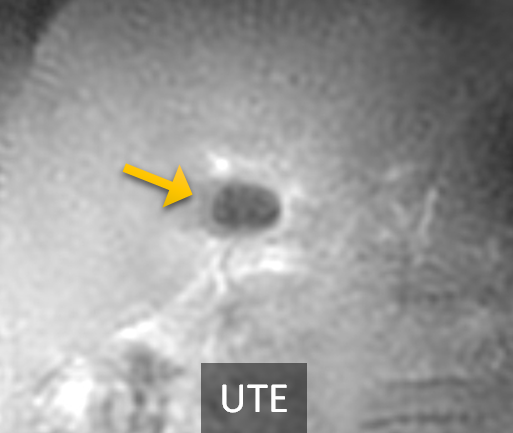
UTE
CASE 59y.o female with a cholesterol gallstone A stone could be visualized as low signal on T1WI. Even on UTE image the signal was weak, but on Subtraction image it could be clearly visualized as positive signal.
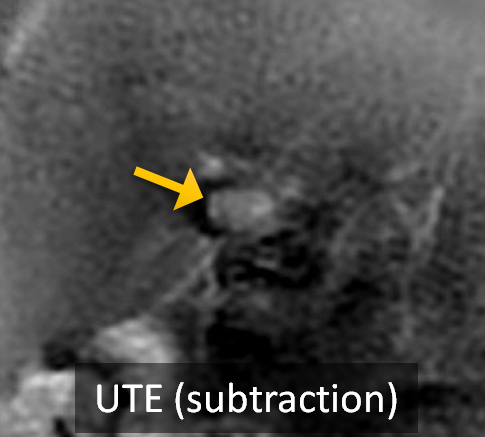
UTE (SUBTRACTION)
CASE 59y.o female with a cholesterol gallstone A stone could be visualized as low signal on T1WI. Even on UTE image the signal was weak, but on Subtraction image it could be clearly visualized as positive signal