2042
Test-Retest Repeatability of MR Elastography (MRE) Stiffness Measurements of Liver Phantoms1Radiology, Mayo Clinic, Rochester, MN, United States
Synopsis
All the previous test-retest human liver MRE studies could involve physiological stiffness change . In this study, our goal was to evaluate MRE test-retest repeatability with liver phantoms to avoid the possible influence of physiological changes in humans. We hypothesized that the variations of test-retest MRE stiffness measurements of phantoms were smaller than that of human livers.
Background
Chronic liver disease, such as chronic hepatitis C infection and nonalcoholic steatohepatitis, is a leading cause of death in the United States[1]. For the vast majority of affected patients, the morbidity and mortality from chronic liver disease and cirrhosis are directly related to progressive hepatic fibrosis. Therefore, it is important to longitudinally monitor disease progression for patient management and treatment efficacy evaluation.
Test-retest repeatability of liver stiffness measurements is a key parameter to characterize MRE system variations for longitudinal disease monitoring. In a MRE study of 5 healthy subjects and 5 HCV-infected patients (F2-F4), the within-subject coefficient of variation (CV) was 6.27-11.00% (between-day, 1-2 weeks apart) and 3.17-8.43% (within-day)[2]. In a MRE study of 20 healthy volunteers (scanned twice on the same day, then twice again 2-4 weeks later) and 10 patients (twice on the same day), the standard deviation of the difference between two longitudinal measurements was 17.4%. The authors concluded that changes greater than 37.0% of the smaller measured stiffness value represent meaningful changes in longitudinal liver stiffness measurements[3]. All of these test-retest human studies could involve physiological stiffness change that is hard to eliminate from the measurement variations.
Therefore, in this study, our goal was to evaluate MRE test-retest repeatability with liver phantoms to avoid the possible influence of physiological changes in humans. Our hypothesis was that the variations of test-retest MRE stiffness measurements of phantoms were smaller than that of humans.
Method
Liver Phantom: The MRE liver phantoms were made of Polyvinyl Chloride (PVC) in a cylindrical container 12.5-cm high and 15.5-cm in diameter. Three phantoms were made with different stiffnesses: soft, medium and hard. A commercially available liver MRE driver was mounted on top of the phantom while the phantom was positioned vertically and an elastic belt was used to secure them to each other. A commercially available GE 8-channel RF coil array (GE Healthcare, Waukesha, WI) was used to image the phantom with some cushions positioned around the phantom so that the coil was separated from the phantom vibrations during the MRE scan.
Imaging Parameters: A 1.5-T whole-body MR imaging system (GE Signa HDxt, GE Healthcare, Waukesha, WI) was used to scan the phantom, and a GRE MRE sequence was used with the following major parameters: imaging plane = coronal, slice thickness = 10 mm, FOV = 20 cm, acquisition matrix = 256x64, TE = 18.6 ms, TR = 50 ms, flip angle = 25º, bandwidth = 31.25 kHz, parallel imaging acceleration factor = 1, driver power = 10%, driver frequency = 60 Hz, driver cycles = 3, motion-encoding-gradient (MEG) frequency = 75 Hz, MEG amplitude = 3 G/cm. A circular ROI was drawn in the middle of the phantom with a diameter half that of the phantom and transferred onto the elastograms. The edges of the phantom were excluded from the ROI due to edge artifacts in the MRE processing. The mean and standard deviation of the pixel values in the ROI were reported (in units of Pa or kPa).
Test-Retest Repeatability: For each of the 3 phantoms, after the first MRE examination was performed, the RF coil and MRE driver were removed and the phantom was taken out. The phantom was re-setup for a 2nd MRE examination and taken out again. The same procedure was repeated to get 10 examinations in total. The time interval between each examination was about 5 minutes.
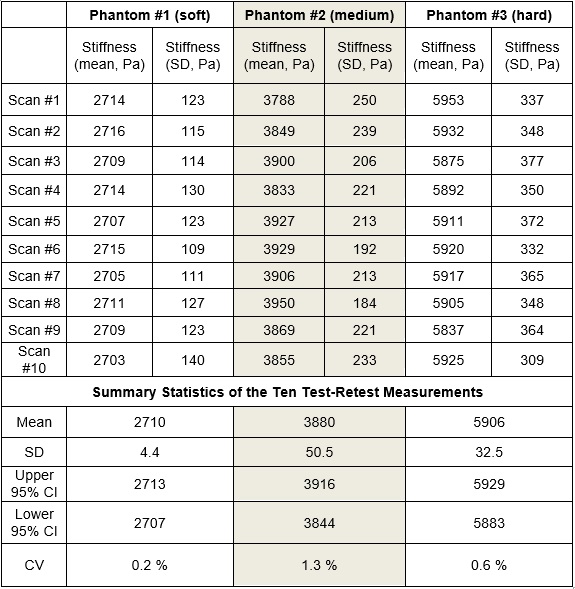
Statistical Analysis: For each of the 3 phantoms, the 10 test-retest measurements were used to determine the mean, standard deviation (SD), coefficient of variation (CV, SD/mean), and 95% confidence intervals (CI).
Results and Discussion
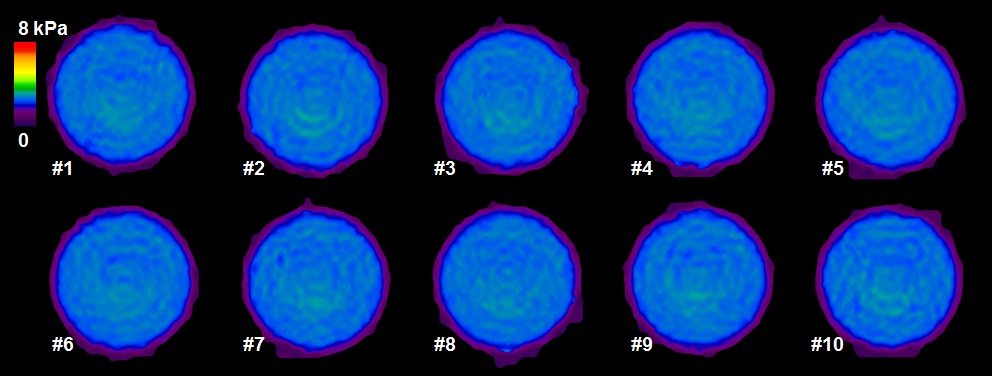
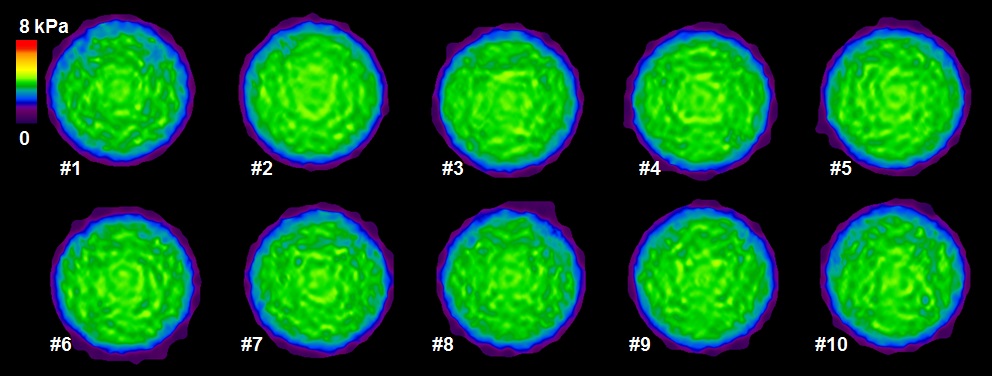
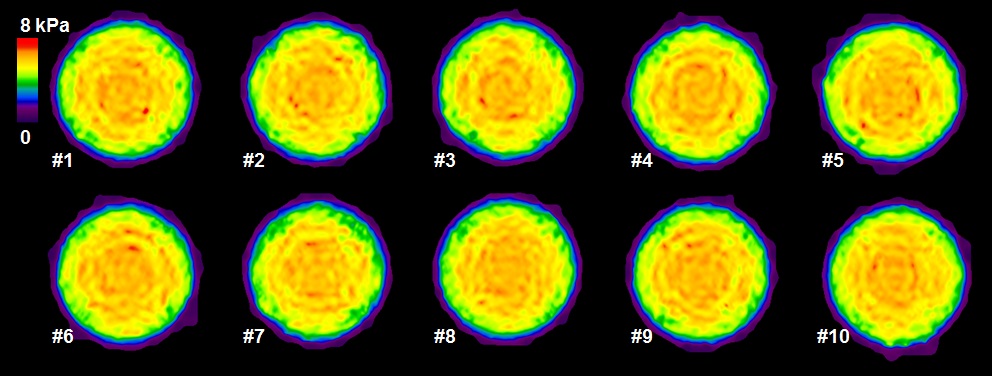
Figures 1, 2 and 3 show the elastograms of the 10 test-retest MRE measurements of the soft, medium and hard phantoms, respectively. We found among the 10 test-retest measurements, the CV was very small: 0.2%, 1.3% and 0.6% for the soft, medium and hard phantom, respectively (Figure 4).
The test-retest repeatability of phantom MRE stiffness measurements was much higher than that of the literature report for human beings. This could be because the phantoms were less like to change stiffness in such a short time period, unlike liver stiffness which may be influenced by human physiology, driver placement and breath-hold locations. The procedure implemented in our current study is more designed to test the “true” MRE system variation without the physiological influence.
Conclusion
By removing the possible effects of breath-hold and driver placement variations and physiological variations of the liver itself over time, the test-retest repeatability of MRE stiffness measurements of liver phantoms was better than that of human livers.Acknowledgements
NIH EB 001981References
1. AHRQ, Healthcare Costs Utilization Project online datebase, in http://hcup.ahrq.gov/HCUPNet.asp2009, U.S. Department of Health & Human Services.
2. Shire, N.J., et al., Test-retest repeatability of MR elastography for noninvasive liver fibrosis assessment in hepatitis C. Journal of magnetic resonance imaging : JMRI, 2011. 34(4): p. 947-55.
3. Hines, C.D., et al., Repeatability of magnetic resonance elastography for quantification of hepatic stiffness. Journal of magnetic resonance imaging : JMRI, 2010. 31(3): p. 725-31.
Figures