2041
Initial Experience of MR Elastography Using Spatially Selective Excitation for the Pancreas.1Diagnostic Radiology & Nuclear Medicine, Hamamatsu University school of Medicine, Shizuoka, Japan, 2Fundamental Development for Advanced Low Invasive Diagnostic Imaging, Nagoya University Graduate School of Medicine, Nagoya, Japan, 3Radiology, Hamamatsu University Hospital, Shizuoka, Japan, 4GE Healthcare Japan, Tokyo, Japan
Synopsis
We tried reduced-FOV MR elastography using a local excitation technique called FOCUS for the pancreas. Comparing conventional-MRE with FOCUS-MRE, there was no significant differences of the measurable are of pancreas. In both methods, the higher the body mass index was, the smaller the measurable area of the pancreas.
Introduction
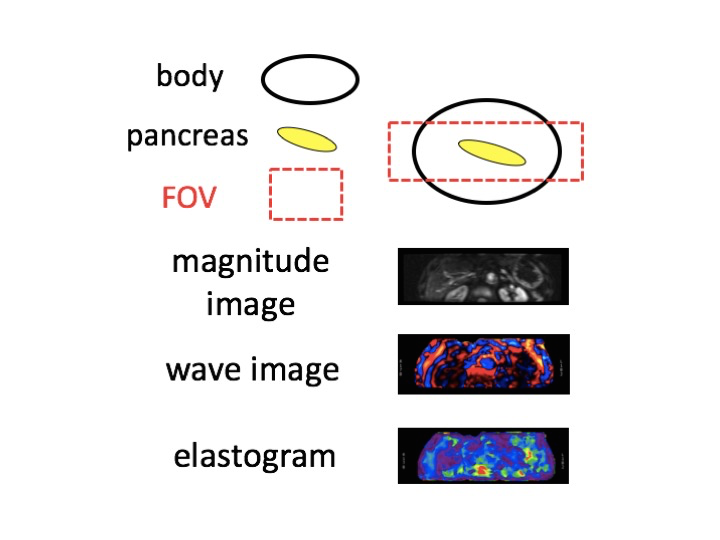
The pancreas is small in size compared to the size of the abdomen; therefore, the reduction of FOV may benefit single shot EPI-based MR Elastography (MRE). However, simple reduction of the FOV will create mis-registration of excited frequencies and aliasing artifacts. One of the solution to this problem is to use 2D RF excitation that is spatially selective in the slice selective as well as phase encoding direction to excite a limited phase FOV1. Previous investigators have reported that the combination of SS-SE-EPI with a spatially selective excitation efficiently reduced FOV in the phase encoding direction without wrap around artifacts, thereby increased the spatial resolution for the renal MRE without problematic artifacts2. This local excitation technique is called FOCUS (FOV Optimized and Constrained Undistorted Single-shot), so we call this combined MRE method FOCUS-MRE. In this study, we report a use of FOCUS-MRE on the pancreas as an initial clinical use of the technique in comparison to the conventional-MRE.Purpose
The purpose of this study was three-fold.
1) To test if newly developed FOCUS-MRE is applicable to the pancreatic assessment.
2) To compare the measurable area (non cross-hatched area) between conventional-MRE and FOCUS-MRE for the pancreatic MRE.
3) To investigate the factors that affect the cross-hatches over pancreas in MRE with both methods.
Materials & Methods
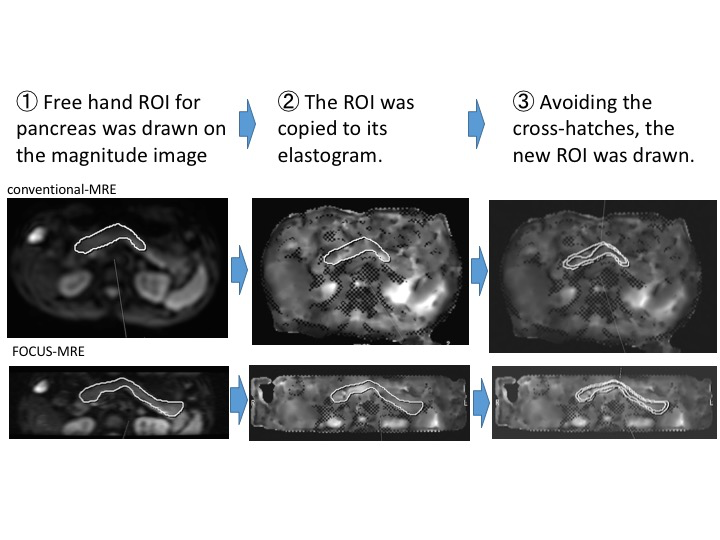
Consecutive 19 patients (10 men and 9 women, age ranging from 41 to 81 years, median age of 74) who were suspected to have pancreatic diseases underwent pancreatic MRE after giving written informed consent. All examinations were conducted on a 3.0-T MR unit (Discovery 750w, GE Healthcare, Milwaukee, WI) with body phased array coil with 32 elements. Pneumatic driver was placed on the anterior abdominal wall after upper abdomen was braced with elastic band. A spin-echo based echo planar MRE was utilized with motion encoding gradients of 60 or 80Hz, motion-encoding gradients direction = z, external driver frequency/amplitude of 60Hz/50% and temporal phase of 4. In both cases, six 7-mm thick slices were acquired in two 12s breath-holds. The wave image and elastogram were automatically generated by MR-Touch system. Other parameters were FOV of 40x40cm, Matrix of 64x64 (conventional-MRE), variable FOV(average size 33x8cm; including both lateral side of patients body, ventral and dorsal areas of the pancreas was reduced)(Figure1), and Matrix of 64x64(FOCUS-MRE). Free hand ROI for pancreas was drawn on the magnitude image and copied to its elastogram. Then, avoiding cross-hatches, new ROI was drawn (Figure2). The percentage of measurable areas were calculated and compared between conventional-MRE with FOCUS-MRE.Then, patients BMI and estimated pancreatic volume were analyzed with the ratio of measurable pancreatic area.Results
1) FOCUS-MRE was successfully applied to the pancreatic examination. None of the problematic artifacts such as aliasing or mis-registrations were discerned with reduced FOV.
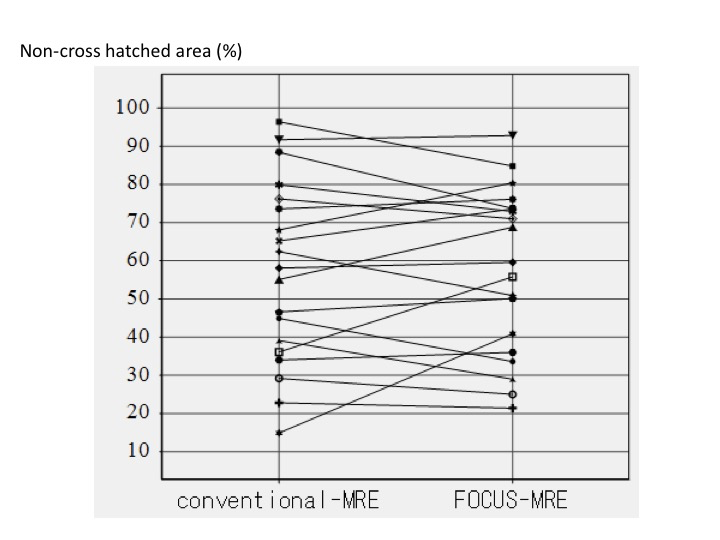
2) In both MRE methods, there were no significant differences concerning the percentage of the measurable area on the pancreas reflected by non-cross hatched area (Figure3).
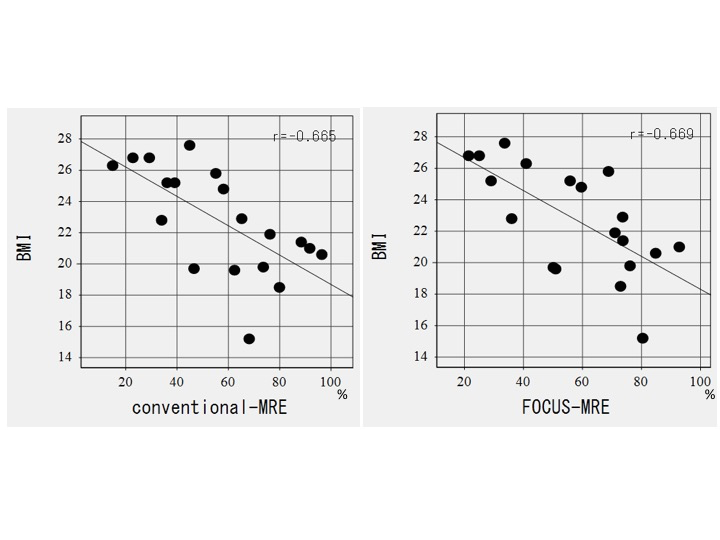
3) The higher the body mass index (BMI), the smaller the measurable area of the pancreas (conventional-MRE : r = -0.67 (p <0.01) , FOCUS-MRE : r = -0.67 (p <0.01)) (Figure4). There was no correlation between pancreatic volume with the ratio of measurable pancreatic area.
Conclusion
The FOV reduction was feasible in pancreatic MRE using FOCUS without any problematic artifacts. There was no significant differences in their percentages of measurable area on the pancreas. In both MRE methods, measurable areas were significantly affected by patients obesity reflected by BMI.Acknowledgements
No acknowledgement found.References
1. Alley M, Pauly JM, Sommer FG, et al. Angiographic imaging with 2D RF pulses. Magn Reson Med. 1997;37:260–267.
2. Ozaki M, et al. MR Elastography using SS-SE-EPI with reduced FOV for Kidney: Preliminary Study. Joint Annual Meeting ISMRM-ESMRMB 2014 10-16 May 2014, Milan, Italy
Figures