2038
Abdominal Fast Advanced Spin Echo Diffusion-Weighted Imaging1Advanced Biomedical Imaging Research Center, Kobe University Graduate School of Medicine, Kobe, Japan, 2Center of Radiology and Radiation Oncology, Kobe University Hospital, Kobe, Japan, 3Toshiba Medical Systems Corporation, Otawara, Japan, 4Radiology, Kobe University Graduate School of Medicine, Kobe, Japan
Synopsis
To reduce distortion on abdominal EPI-DWI, we developed Fast Advanced Spin Echo (FASE)-DWI for abdominal 3T imaging. FASE-DWI improved distortion and showed equivalent diagnostic performance and be used as an alternative to EPI-DWI.
INTRODUCTION & PURPOSE
In current abdominal MRI, DWI is one of the most important techniques and routinely used worldwide.
However, problems still remain such as poor image quality and distortion due to air in lung or intestinal, or outside the body, especially when using single-shot EPI at 3T.
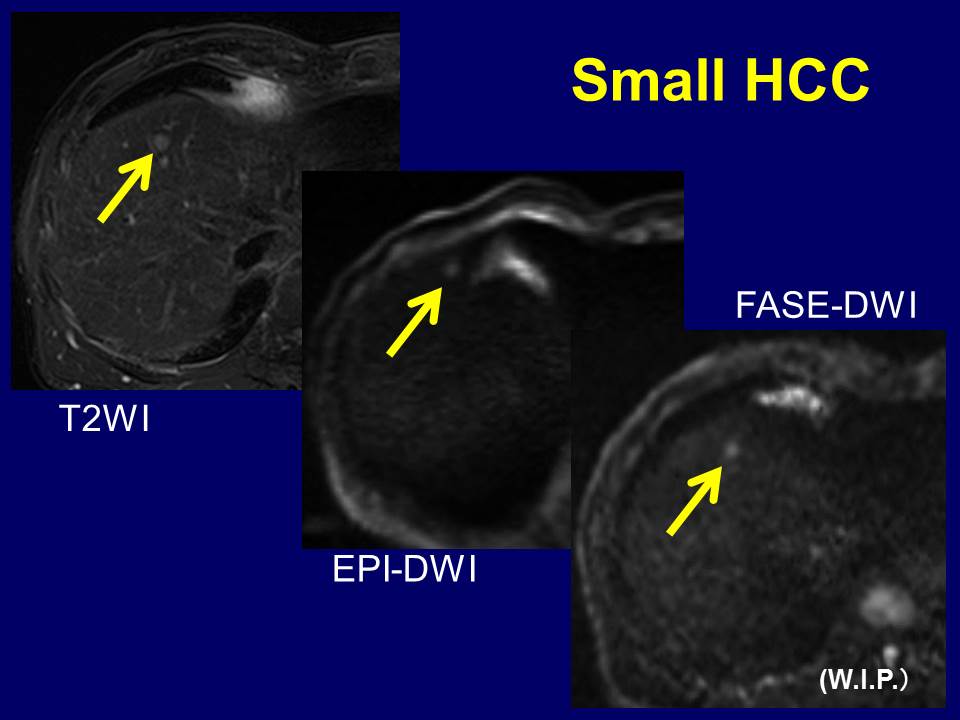
To solve this problem, we developed Fast Advanced Spin Echo (FASE)-DWI (W.I.P.)for abdominal 3T imaging.
The purpose of this study was to assess FASE-DWI in evaluation of abdominal diseases.
MATERIALS & METHODS
Subjects
•70 patients (44 men and 26 women, mean: 68.4 years) who were suspected to have malignant tumor in the liver, bile duct (BD), or pancreas underwent MR examination at a 3T scanner were enrolled.
•Malignant lesions were confirmed in 18 HCC, 3 IHCCC, 5 metastatic liver, 4 extrahepatic cholangiocellular, 5 pancreatic, and 4 LN metastatic cancer patients.
Imaging Technique
•Vantage Titan 3T (Toshiba Medical Systems Co.)
•EPI-DWI TR/TE/FA=6500-10000/70/90, b values: 0 & 1000, matrix: 128×120, thickness: 8mm, NEX: 4, scan time: 3-6min, PASTA+SPAIR, PI: 2.0, MPG: (y, z)
•FASE-DWI (W.I.P.) TR/TE/FA=10000/80/90, b values: 0 & 600, matrix: 112×96, thickness: 8mm, NEX: 5, scan time: 6:20min, SPAIR, PI: 2.0, MPG: (x, y, z)
Quantitative Assessments
•Antero-posterior (AP) and right-to-left (RL) abdominal diameters were measured on the slice with most severe image distortion for each sequence and each patient.
•Correlation analyses among EPI-DWI, FASE-DWI, and T2WI were performed.
•ADCs in malignant lesions and background organs were measured on FASE and compared.
Qualitative Assessments
•Amount of abdominal gas and ascites on images was recorded for each patient using a 5-point scale (1:no, 5: massive).
•Overall image quality and severity of image distortion were visually assessed using a 5-point scale (1:poor/none, 5: excellent/severe) on EPI-DWI and FASE-DWI, and compared.
•Regression analyses were done to estimate factors for low image quality and severe distortion.
•Malignant lesion detection and lesion conspicuity were separately assessed on EPI and FASE and compared. ROC analysis was used for lesion detection.
RESULTS
Quantitative
•Correlation coefficient was highest between T2WI and FASE for both the diameters. Coefficient was lowest in AP on EPI.
•Mean ADC in lesions was significantly lower than that in backgrounds (1.63 vs 2.17x10-6, p< 0.0001).
Qualitative
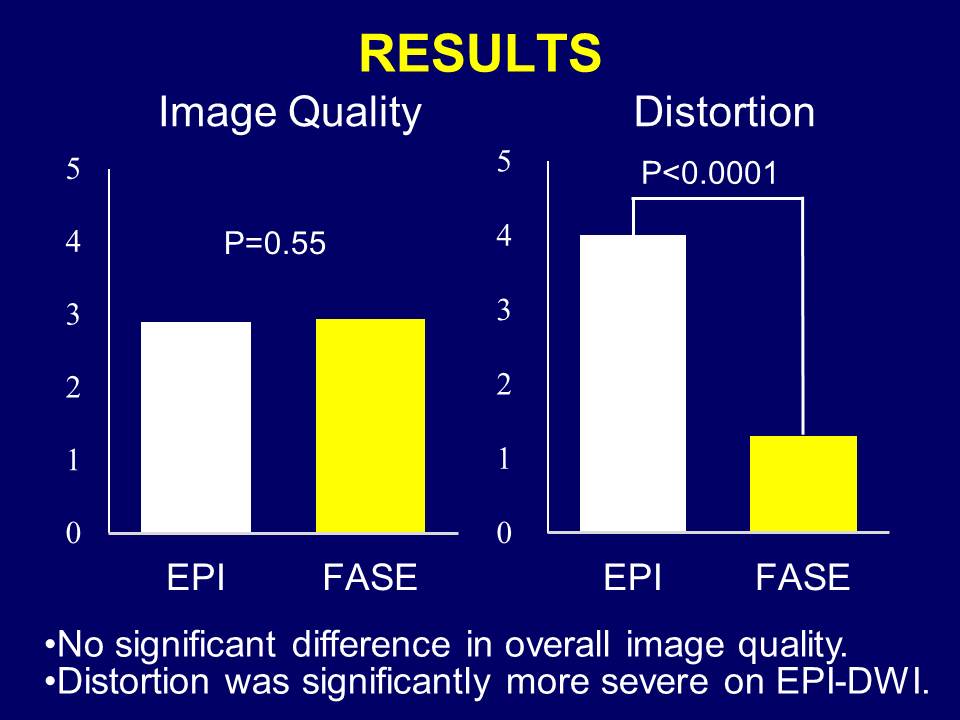
•There was no significant difference between overall image qualities.
•Image distortion was significantly more severe on EPI.
•Sex and gas were found to be significant factors for image quality and distortion on EPI, and sex was a significant factor for image quality on FASE.
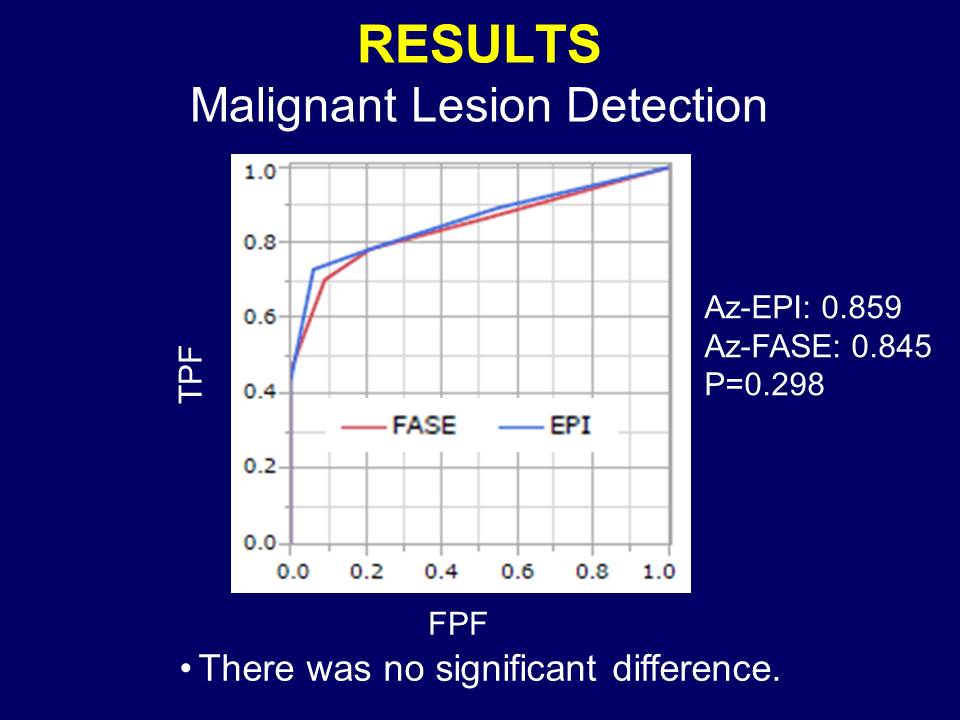
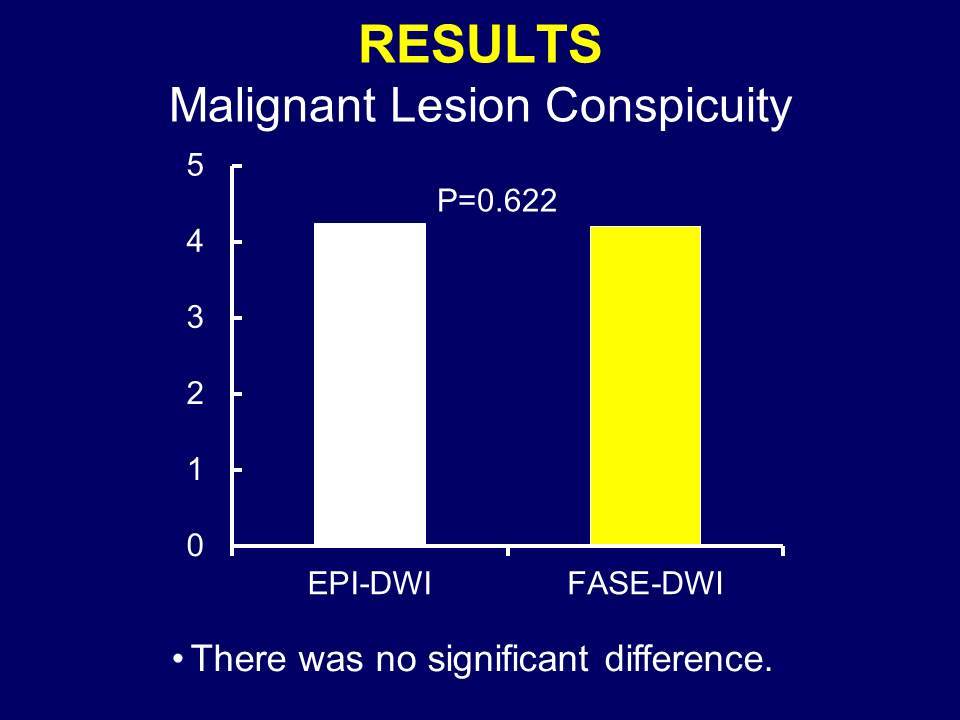
•There was no significant difference in malignant lesion detection (Az-EPI: 0.859, Az-FASE: 0.845, p=0.298) and conspicuity (EPI: 4.24, FASE: 4.20, 0.689).
DISCUSSION
•Distortion was reduced on FASE-DWI.
•No significant deference in image quality.
•Image quality and distortion on EPI-DWI were significantly affected by abdominal gas.
•Diagnostic performance and conspicuity for malignant lesions are similar both on EPI-DWI and FASE-DWI.
•FASE-DWI was useful in the abdominal parts near air.
CONCLUSION
Abdominal FASE-DWI can improve image quality and decrease image distortion without hampering lesion detection and ADC measurement.Acknowledgements
No acknowledgement found.References
•Ohno Y, et al. EJR 2015 (Lung CA, N-staging)
•Kito S, et al. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006(head & neck abscesses)
Figures