2035
Free-Breathing Hepatobiliary Phase Imaging: Comparison of Five Free-Breathing Scans with Conventional Breath Hold Scan1Radiology, Gifu University Hospital, Gifu City, Japan, 2Philips Healthcare, Tokyo, Japan, 3Philips Electronics Japan, Tokyo, Japan
Synopsis
We applied five free-breathing scan sequences to gadoxetic acid-enhanced hepatobiliary phase imaging. Breath hold eTHRIVE demonstrated the highest SNR on the liver, although it is also revealed the disadvantage for the patients with unstable breath hold. On the other hand, free-breathing 3D VANE with gate and track demonstrated the highest image quality with equivalent SNR to breath hold eTHRIVE. It is notable that free-breathing 3D VANE produced steady and effective image quality for all patients regardless of breath hold ability.
Purpose
Gadoxetic acid MRI contrast medium enables initial hemodynamic imaging and then liver-specific hepatobiliary phase imaging. The hepatobiliary phase imaging is especially excellent for the differentiation between lesions with and without functional hepatocytes and now widely used in clinical imaging (1, 2). Now, fat-suppressed three-dimensional T1-weighted gradient-echo sequences are widely used for the breath holding dynamic and hepatobiliary phase imaging, whereas we often experienced a certain number of patients with unstable breath hold. Recently, several free-breathing sequences were feasible for whole-liver imaging and gradually introduced in clinical imaging (3, 4). So the purpose of this study was to assess the five free-breathing scan techniques for gadoxetic acid-enhanced hepatobiliary phase imaging compared with conventional breath hold scan.Materials and Methods
Fourteen-patients (7 men and 7 women, mean age: 67.4 years, age range; 43–79 years) underwent gadoxetic acid-enhanced MR imaging for the evaluation of suspected liver tumor. All examinations were performed using a 3T clinical scanner (Ingenia CX, Philips Healthcare) with a MultiTransmit RF system and a 32 channel phase-array receiver coil. Hepatobiliary phase images were obtained by the following six scans including fat-suppressed three dimensional T1-weighted turbo field echo (eTHRIVE) and that with golden-angle radial stack-of-stars acquisition (3D VANE) (5): 3D VANE with gate and track (VANEG&T), 3D VANE with track (VANET), 3D VANE without gate and track (VANE), thin-slice 3D VANE with gate and track (Thin-VANEG&T), eTHRIVE without breath hold (eTHRIVEFB), and eTHRIVE with breath hold (eTHRIVEBH) (Table 1). Quantitative and qualitative analyses were performed by two blinded radiologist. Signal intensity of the liver (SILiver) and paraspinal muscle (SIMuscle), and standard deviation (SDLiver) were calculated using circular region-of-interest (ROI) for the quantification of SNR (SNRLiver = SILiver / SDLiver / SIMuscle). Image quality was evaluated using 5-point scale regarding sharpness, motion artifact, visibility of intrahepatic vessels, and overall image quality. SNRLiver and image quality were compared between six scan sequences.Results
eTHRIVEBH demonstrated the highest SNRLiver which was marginally higher than VANET (P = 0.07), VANE (P = 0.05), and Thin-VANEG&T (P = 0.06). No significant difference was found in SNRLiver between eTHRIVEBH, eTHRIVEFB, and VANEG&T (P = 0.12–0.82) (Figure 1). Thin-VANEG&T showed the highest image quality followed by VANEG&T regarding sharpness, motion artifact, visibility of intrahepatic vessels, and overall image quality (P < 0.001) (Figure 2). Severe motion artifacts were observed in one and 10 patients in eTHRIVEBH and eTHRIVEFB, respectively, while image quality kept above acceptable range in VANEG&T, VANET, VANE, and Thin-VANEG&T (Figure 3).Discussion
Breath hold eTHRIVE demonstrated the highest SNR on the liver, although it is also revealed the disadvantage for the patients with unstable breath hold. On the other hand, free-breathing 3D VANE with gate and track demonstrated the highest image quality with equivalent SNR to breath hold eTHRIVE. It is notable that free-breathing 3D VANE produced steady and effective image quality for all patients regardless of breath hold ability. In conclusion, free-breathing 3D VANE with gate and track was feasible for free-breathing hepatobiliary phase imaging. It can be applied to the supplemental sequence to cover the patients with unstable breath hold.Acknowledgements
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.References
1. Kitao A, Zen Y, Matsui O, et al. Hepatocellular carcinoma: signal intensity at gadoxetic acid-enhanced MR Imaging--correlation with molecular transporters and histopathologic features. Radiology. 2010;256(3):817-26.
2. Sano K, Ichikawa T, Motosugi U, et al. Imaging study of early hepatocellular carcinoma: usefulness of gadoxetic acid-enhanced MR imaging. Radiology. 2011;261(3):834-44.
3. Chandarana H, Block KT, Winfeld MJ, et al. Free-breathing contrast-enhanced T1-weighted gradient-echo imaging with radial k-space sampling for paediatric abdominopelvic MRI. Eur Radiol. 2014;24(2):320-6.
4. Bamrungchart S, Tantaway EM, Midia EC, et al. Free breathing three-dimensional gradient echo-sequence with radial data sampling (radial 3D-GRE) examination of the pancreas: Comparison with standard 3D-GRE volumetric interpolated breathhold examination (VIBE). J Magn Reson Imaging. 2013;38(6):1572-7.
5. Winkelmann S, Schaeffter T, Koehler T, Eggers H, Doessel O. An optimal radial profile order based on the Golden Ratio for time-resolved MRI. IEEE Trans Med Imaging. 2007;26(1):68-76.
Figures
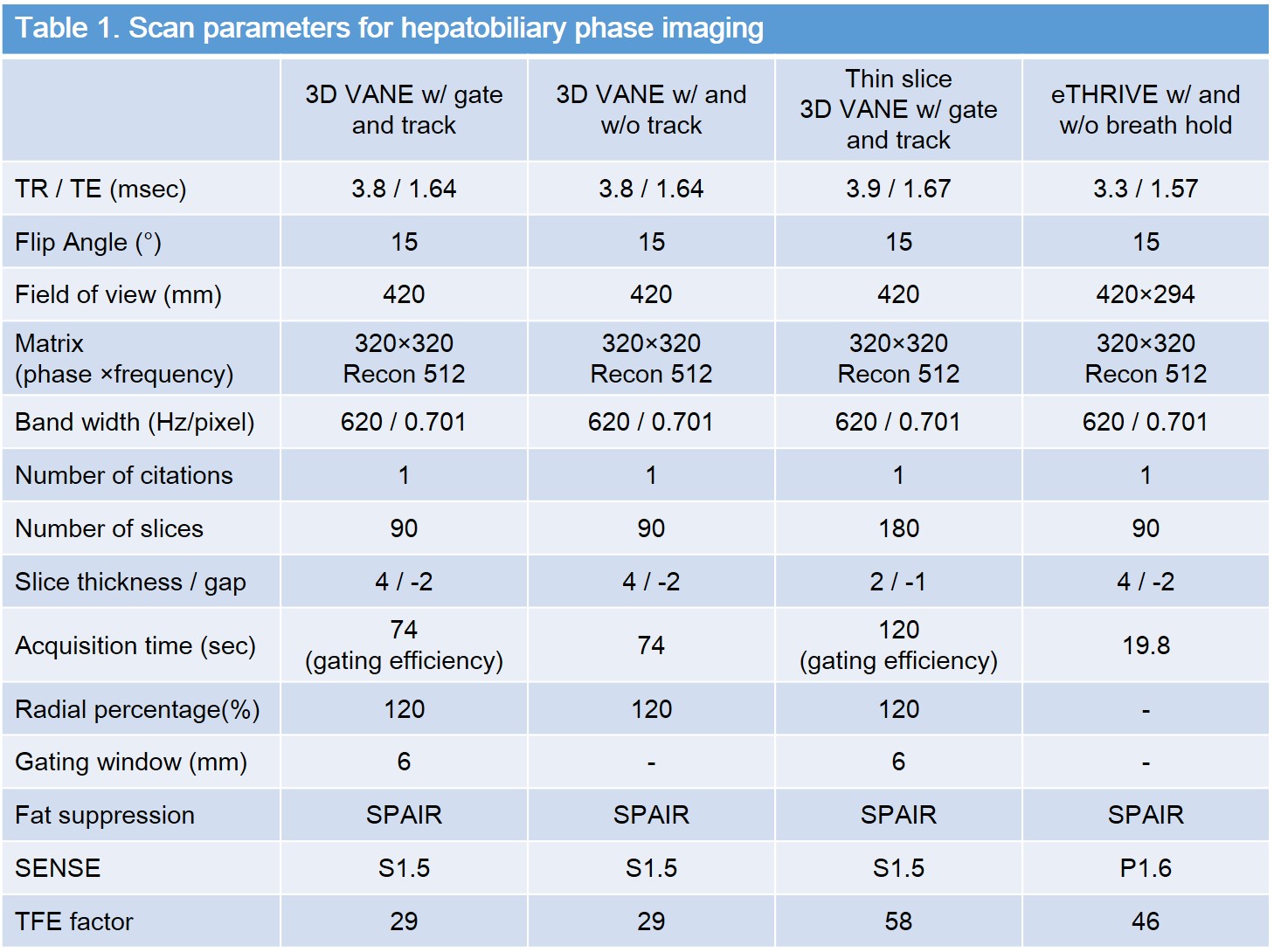
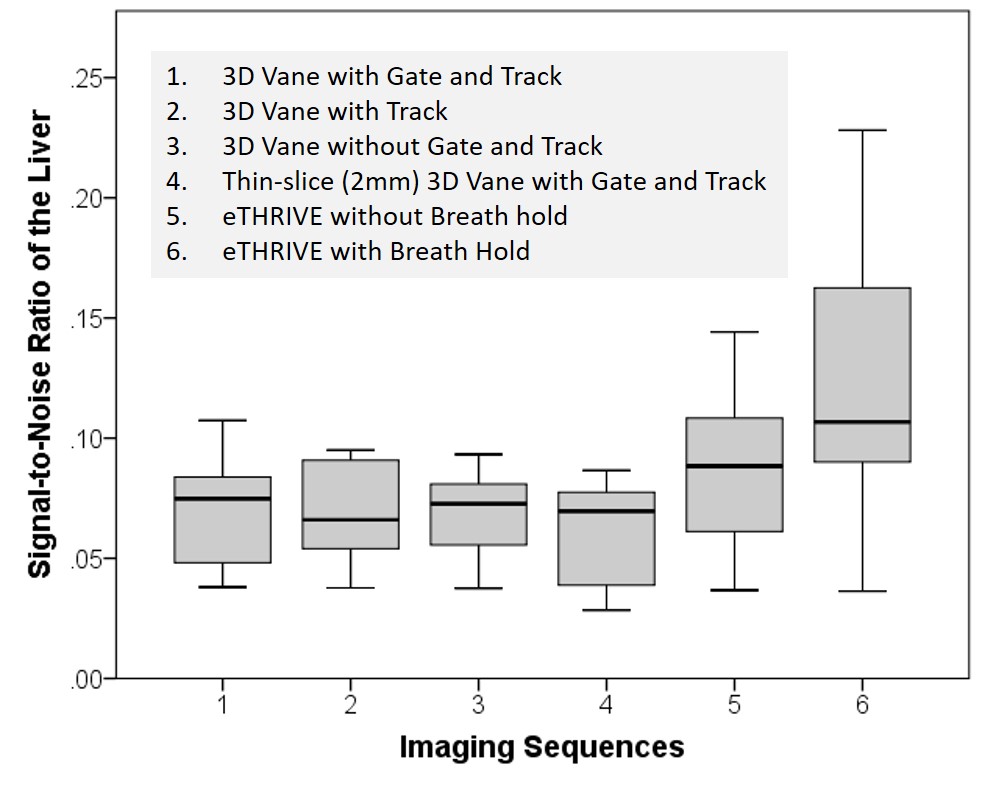
Figure 1. Signal-to-noise ratio of the liver in each sequence.
eTHRIVEBH demonstrated the highest SNRLiver which was marginally higher than VANET (P = 0.07), VANE (P = 0.05), and Thin-VANEG&T (P = 0.06). No significant difference was found in SNRLiver between eTHRIVEBH, eTHRIVEFB, and VANEG&T (P = 0.12–0.82)
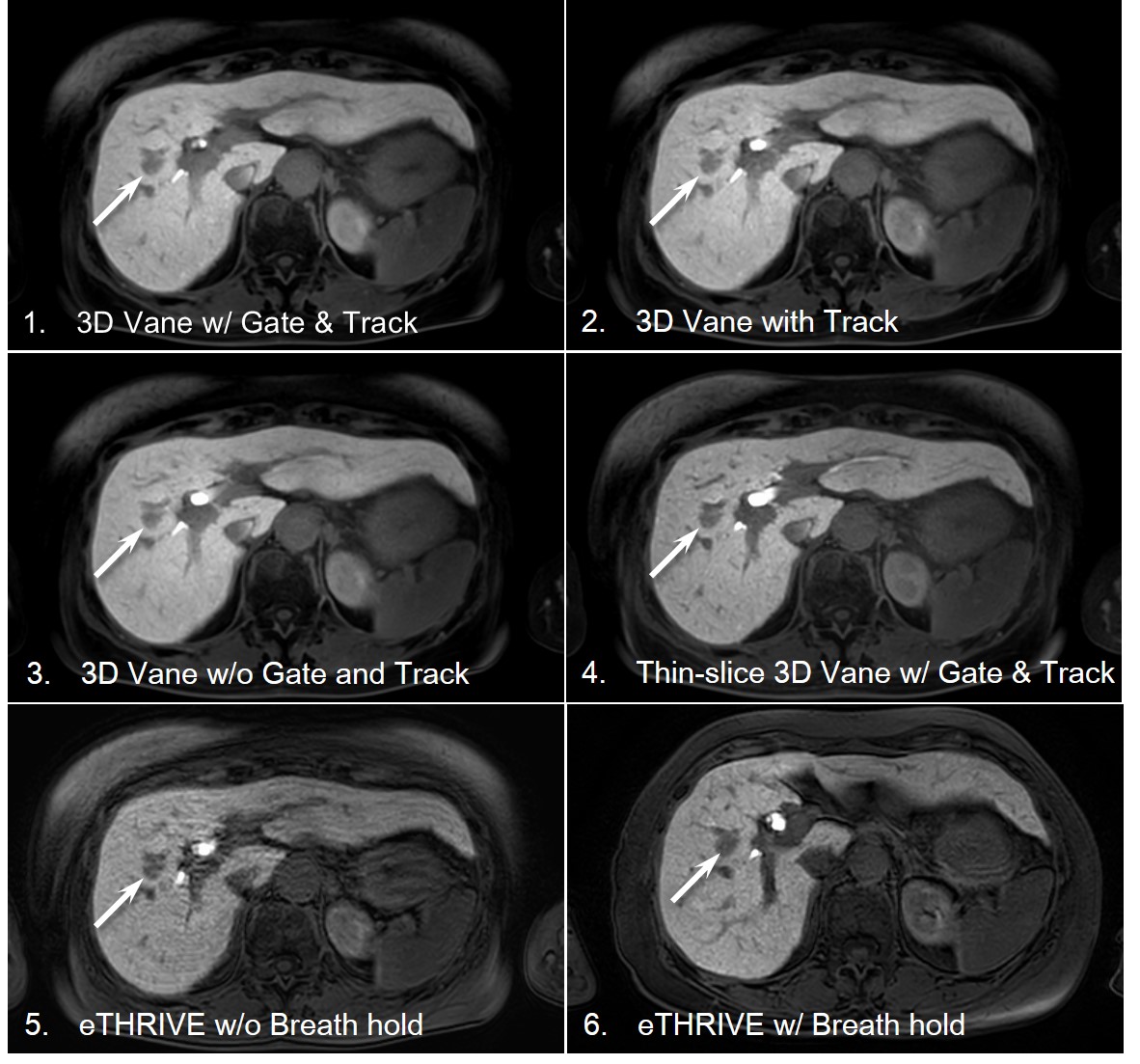
Figure 2. A 77 year-old man with chronic hepatitis C and hepatocellular carcinoma (HCC).
Thin-VANEG&T demonstrated the equivalent image quality to eTHRIVEBH. Low intensity area corresponding to HCC was seen in all sequences (arrow).
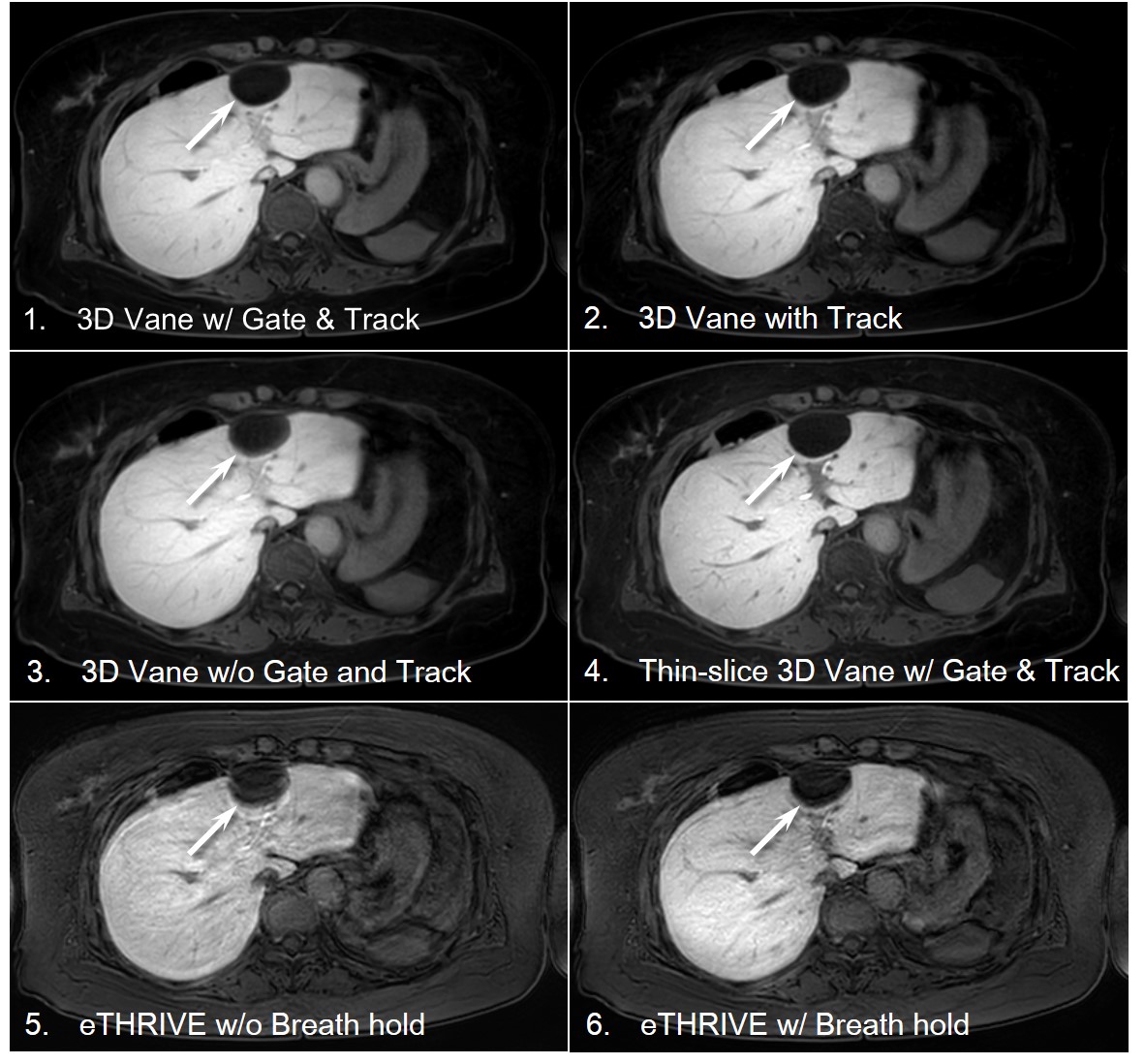
Figure 3. A 62 year-old woman with chronic hepatitis B and simple cyst.
Thin-VANEG&T demonstrated the the highest image quality superior to eTHRIVEBH. Low intensity area corresponding to a cyst was seen in all sequences (arrow).