2034
Comprehensive dynamic contrast-enhanced 3D MR imaging of the breast with fat/water separation and high spatiotemporal resolution using Dixon Radial Volumetric Encoding (Dixon-RAVE)1Center for Advanced Imaging Innovation and Research (CAI2R), Department of Radiology, New York University School of Medicine, New York, NY, United States, 2Bernard and Irene Schwartz Center for Biomedical Imaging, Department of Radiology, New York University School of Medicine, New York, NY, United States
Synopsis
Conventional clinical breast MRI consists of several separate T1-weighted scans, including both pre-contrast fat-suppressed and non-fat-suppressed acquisitions as well as the acquisition of dynamic contrast-enhanced phases.
Here, we show how this entire exam can be replaced by a single comprehensive scan, therefore reducing overall scan time and simplifying the clinical workflow. This is achieved by using radial stack-of-stars sampling in combination with a model-based fat/water separation technique, which takes into account the off-resonant blurring of fat and integrates both compressed sensing and parallel imaging. The approach is validated in 24 patients and results were evaluated by two radiologists.
Purpose
Dynamic contrast-enhanced (DCE-) MRI is an important tool with high sensitivity for the diagnosis of breast cancer1. To assess tumor morphology and contrast kinetics, both high spatial and high temporal resolution are required. In conventional clinical practice, multiple separate T1-weighted fat-suppressed gradient-echo scans are performed. However, this approach has limitations: 1) Images are acquired with high spatial resolution and, consequently, the achievable temporal resolution is only in the order of 1-3 minutes; 2) The degree of fat suppression can be inhomogeneous across the field-of-view, which can obscure pathologies; 3) An additional non-fat-suppressed scan must be performed to assess fat-containing lesions.
Here, we show how these limitations can be resolved by using the recently proposed Dixon-RAVE technique2. With this approach, only one single continuous scan needs to be performed from which all required T1-weighted contrasts can be extracted, including both a pre-contrast non-fat-suppressed and fat-suppressed image as well as dynamic contrast-enhanced phases with high spatiotemporal resolution.
Methods
Patient study
24 patients (age 51.2±14.9 years) underwent diagnostic bilateral breast DCE-MRI examination on a clinical 3T scanner (Magnetom Trio, Siemens Healthineers). To use the Dixon-RAVE method in this clinical setting without compromising the regular workflow, the sequence was added to the conventional breast protocol as follows: Before injection of contrast agent, both a non-fat-saturated and a fat-saturated T1-weighted Cartesian VIBE scan were performed as part of the clinical protocol. Then, 400 radial projections were continuously acquired for 3:10min using Dixon-RAVE, which is based on a golden-angle stack-of-stars trajectory with blipped bipolar multi-echo readout2. After the first 2min of scanning, gadobutrol (0.1 mM/kg body weight) was injected while the scan was continued. It was immediately followed by acquisition of four conventional fat-saturated Cartesian VIBE images.
Figure 1a summarizes the entire procedure. Acquisition parameters were as follows:
- Non-fat-saturated VIBE scan: TR/TE = 4.74/1.79ms, matrix size = 448x358, FOV = 320x320mm2, resolution = 0.71x0.89x1.10mm3, 192 acquired partitions, acquisition time = 2:19min
- Fat-saturated VIBE scans: TR/TE = 4.74/1.79ms, matrix size = 448x291, FOV = 320x320mm2, resolution = 0.71x0.1.10x1.10mm3, 192 acquired partitions, acquisition time per image = 2:07min
- Dixon-RAVE: TR = 6.54ms, TEs = 1.50/3.12/4.74ms, matrix size = 320x320, FOV = 320x320mm2, resolution = 1.00x1.00x1.20mm3, 144 acquired partitions, slice resolution = 50%, acquisition time = 3:20min
Image reconstruction
All conventional VIBE scans were processed on the scanner with the vendor-provided techniques. Reconstruction of the Dixon-RAVE dataset is schematically shown in Figure 1b. Pre-contrast Dixon-RAVE water and fat images were calculated by retrospectively combining the first 260 projections and performing a model-based reconstruction which includes parallel imaging and deblurring2. Due to the moderate undersampling factor (≈1.9), no additional regularization was employed. To generate the dynamic Dixon-RAVE images, 13 consecutive radial projections were combined for each dynamic frame, resulting in a series of reconstructed fat and water images with a temporal resolution of 6.1s per volume. Because the undersampling factor in this case was ≈38.7, compressed sensing was incorporated by adding temporal total variation as regularization.
Reader evaluation
The following images were rated by two radiologists with 15/7 years of experience on a 5-point scale. Wilcoxon signed rank tests were used for statistical evaluation:
1) Pre-contrast non-fat-suppressed VIBE image and pre-contrast non-fat-suppressed Dixon-RAVE image (generated synthetically by combining the extracted water and fat image)
2) Pre-contrast fat-suppressed VIBE image and pre-contrast water-only Dixon-RAVE image
3) First post-contrast VIBE image and water-only image at the last time point of the dynamic Dixon-RAVE series
Scores were given for overall image quality and conspicuity of fibroglandular tissue from fat. For the fat-suppressed images 1) and 3), the degree of fat saturation was additionally rated. Evaluations from the two radiologists were averaged.
Results
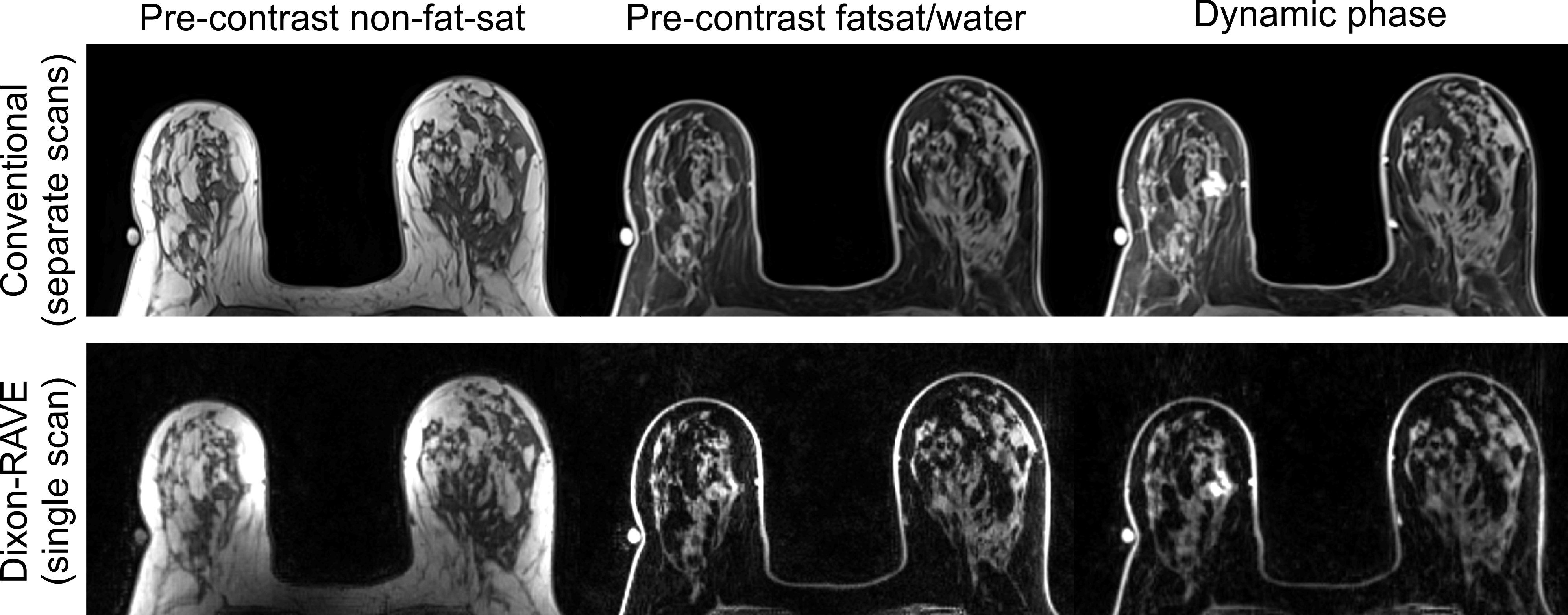
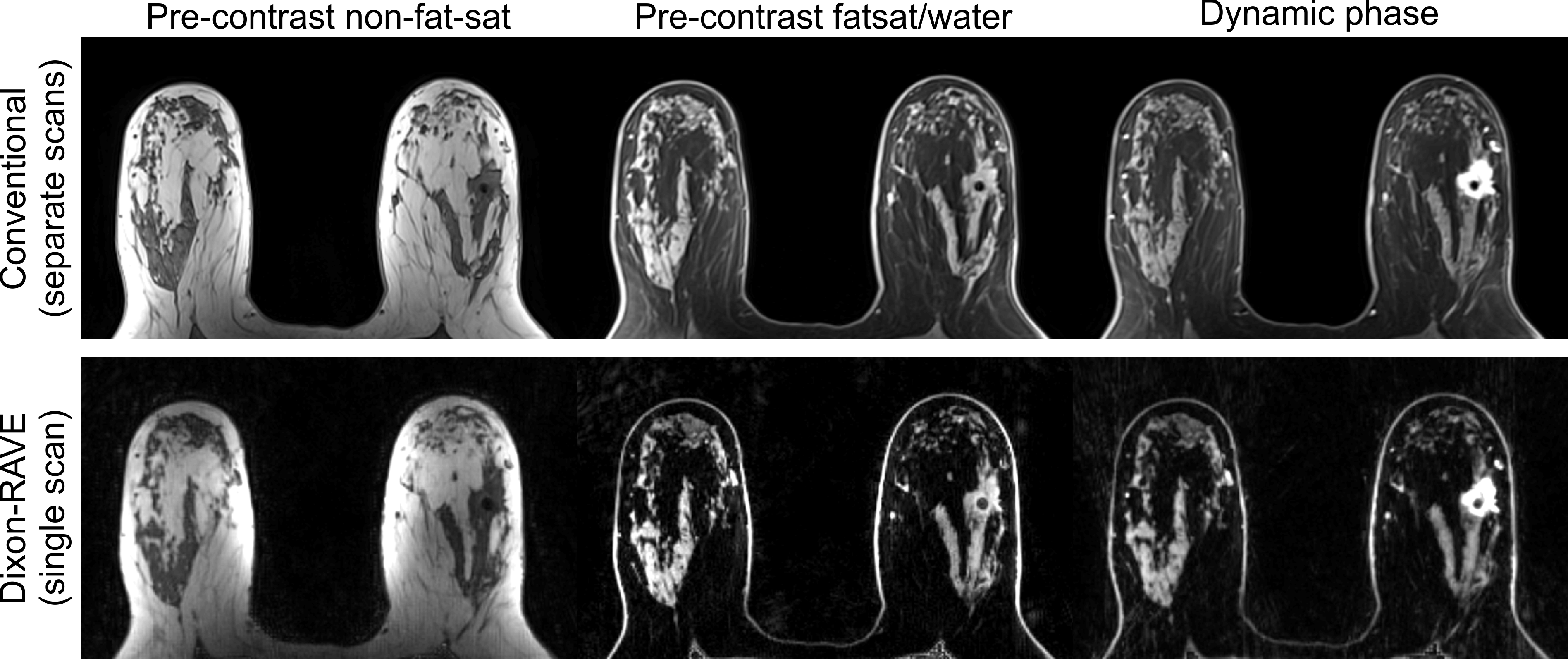
The scores from the reader study are shown in Figure 2. Figures 3 and 4 show results for two patients with breast cancer using the conventional clinical protocol and Dixon-RAVE. Figure 5 shows the entire dynamic image series generated with Dixon-RAVE.Discussion and Conclusion
This work shows that the Dixon-RAVE approach can be used to replace the entire conventional T1-weighted breast examination. While the overall image quality of VIBE is still slightly better than Dixon-RAVE, the proposed approach achieves significantly improved fat suppression. Furthermore, the achievable high spatiotemporal resolution enables assessment of contrast dynamics, which can be of value to predict malignancy of tissue and improves the overall specificity for the diagnosis of breast cancer.
In summary, Dixon-RAVE can serve as a one-stop-shop approach for comprehensive clinical breast imaging, reducing overall scan time and simplifying the clinical workflow.
Acknowledgements
NIH P41EB017183, 5R01EB018308, R01CA160620
References
1. Gilles R et al., Nonpalpable breast tumors: diagnosis with contrast-enhanced subtraction dynamic MR imaging, Radiol, 191:625-631 (1994)
2. Benkert T et al., Free-breathing volumetric fat/water separation by combining radial sampling, compressed sensing, and parallel imaging, Magn Reson Med, 10.1002/mrm.26392 (2016)
Figures
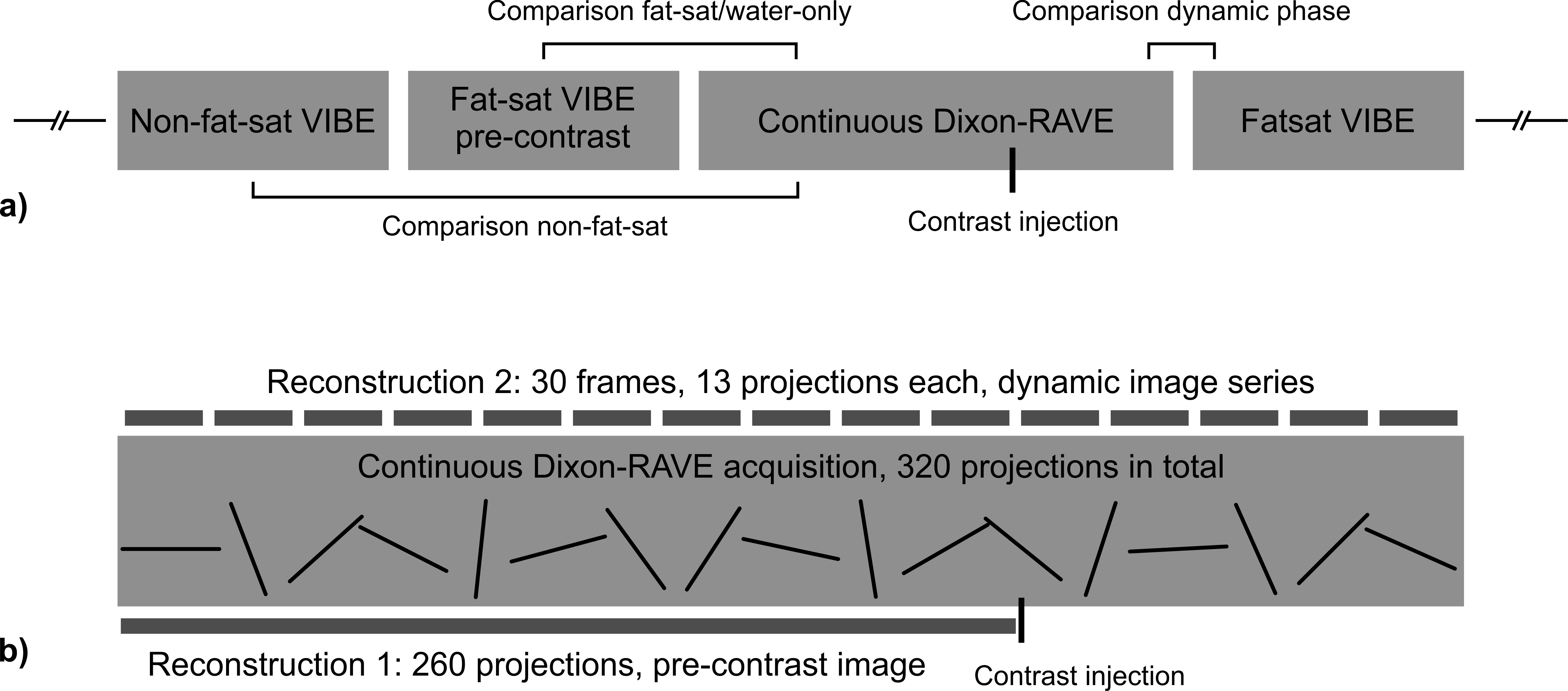
a) Overview of the different scans which were performed for each patient. The brackets indicate which images were compared in the reader study.
b) The Dixon-RAVE dataset was reconstructed in two different ways. 1) A static pre-contrast image was obtained by grouping the first 260 projections, which were acquired before injection of contrast agent (indicated at the bottom). 2) A dynamic series was reconstructed by combining 13 consecutive projections for each frame (indicated at the top).