2011
The value of magnetic resonance elastography in differential diagnosis of hepatocellular carcinoma and intrahepatic cholangiocarcinoma1Imaging Diagnosis, National Cancer Center/Cancer Hospital, Chinese Academy of Medical Science and Peking Union Medical College, beijing, People's Republic of China, 2National Cancer Center/Cancer Hospital, Chinese Academy of Medical Science and Peking Union Medical College
Synopsis
To determine the value of MRE in the differential diagnosis of hepatocellular carcinoma and intrahepatic cholangiocarcinoma with 3.0-T MR scanner . The MRE were performed in 36 patients(26 hepatocellular carcinomas and 11 intrahepatic cholangiocarcinomas) by using 60-Hz mechanical waves and Spin echo echo planar sequence.Intrahepatic cholangiocarcinomas had significantly greater mean shear stiffness than hepatocellular carcinoma (9.08 ±2.13kPa vs 6.54 ±1.84kPa). They have statistically significant differences(p<0.01).MRE can help the differentiation of hepatocellular carcinoma and intrahepatic cholangiocarcinoma.
Introduction
Elasticity is a very important physical property of human tissue. MR elastography (MRE) is a new technique noninvasive assessment of the liver stiffness. Many literature reports that MRE is highly accurate for the diagnosis and staging of liver fibrosis. It is a worthwhile attempt to distinguish the primary malignant tumor of liver such as the hepatocellular carcinoma and intrahepatic cholangiocarcinoma with the hardness measurement of MRE.
Methods
46 patients were performed magnetic resonance elastography (MRE) examination. Imaging was performed on a 3.0-T clinical MR scanner((GE Healthcare, Milwaukee, WI, USA)) equipped with a 32-element phased-array torso coil. The MR elastography were acquired by using 60-Hz mechanical waves and two-dimensional Spin echo echo planar sequence (2D-SE-EPI ). Elastogram was generated in an automated process consisting of an inversion algorithm. Scanning parameters were as follows: TR/TE=600ms/ 50ms, FOV= 38cm×38cm; matrix=64×64;slice thickness= 8mm;spacing=1mm;number of slices= 6~8;bandwidth=256 kHz;scan time 19~21s.11 patients were excluded Because of without histopathological and puncture cytology confirmed. The final study group comprised 35 subjects (31 male, 4 female). One patient has two hepatocellular carcinomas. A total of 26 hepatocellular carcinoma lesions and 11 cholangiocarcinoma lesions Independent sample T test and receiver-operating characteristic curve were performed on the stiffness values for differentiation of hepatocellular carcinomas and intrahepatic cholangiocarcinomas. The background stiffness of the corresponding liver lesions was also compared by independent samples T-testResults
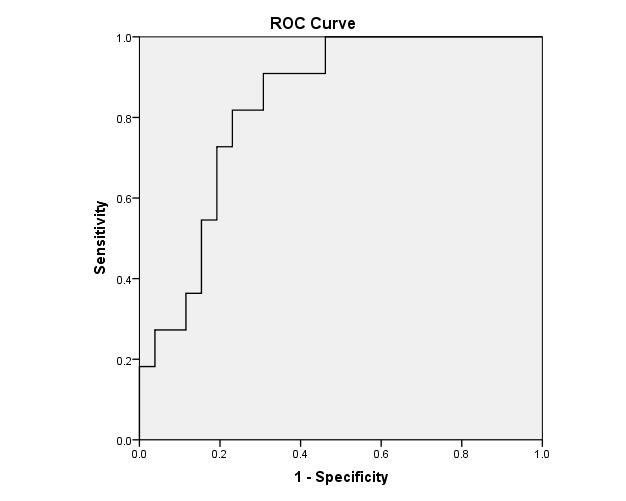
Intrahepatic cholangiocarcinomas had significantly greater mean shear stiffness than hepatocellular carcinoma (9.08 ±2.13kPa vs 6.79 ±1.67kPa)(figure 1). They have statistically significant differences(p<0.01).The area under the receiver-operating characteristic curve is 0.832(figure 2). The background liver stiffness of the hepatocellular carcinoma had significantly greater mean shear stiffness than intrahepatic cholangiocarcinomas (4.48 ±2.07kPa vs 3.53 ±1.34kPa). They have statistically significant differences(p<0.01).Conclusion
MRE can help in the identification of hepatocellular carcinoma and intrahepatic cholangiocarcinoma. The stiffness of the liver in hepatocellular carcinoma is higher than that of intrahepatic cholangiocarcinoma.Acknowledgements
No acknowledgement found.References
1.Liver Stiffness Measurements with MR Elastography: Agreement and Repeatability across Imaging Systems, Field Strengths, and Pulse Sequences. Trout AT, Serai S, Mahley AD, Wang H, Zhang Y, Zhang B, Dillman JR.Radiology. 2016 Jun 10:160209. [Epub ahead of print]
2. Magnetic resonance elastography of liver: technique, analysis, and clinical applications. Venkatesh SK1, Yin M, Ehman RL.J Magn Reson Imaging. 2013 Mar;37(3):544-55.
3. Diagnostic performance of magnetic resonance elastography in staging liver fibrosis: a systematic review and meta-analysis of individual participant data.Singh S, Venkatesh SK, Wang Z, Miller FH, Motosugi U, Low RN, Hassanein T, Asbach P, Godfrey EM, Yin M, Chen J, Keaveny AP, Bridges M, Bohte A, Murad MH, Lomas DJ, Talwalkar JA, Ehman RL. Clin Gastroenterol Hepatol. 2015 Mar;13(3):440-451.
4. MR elastography of liver tumors: preliminary results.Venkatesh SK1, Yin M, Glockner JF, Takahashi N, Araoz PA, Talwalkar JA, Ehman RL.AJR Am J Roentgenol. 2008 Jun;190(6):1534-40.
5. MR elastography of liver tumours: value of viscoelastic properties for tumour characterisation. Garteiser P1, Doblas S, Daire JL, Wagner M, Leitao H, Vilgrain V, Sinkus R, Van Beers BE.Eur Radiol. 2012 Oct;22(10):2169-77.
Figures
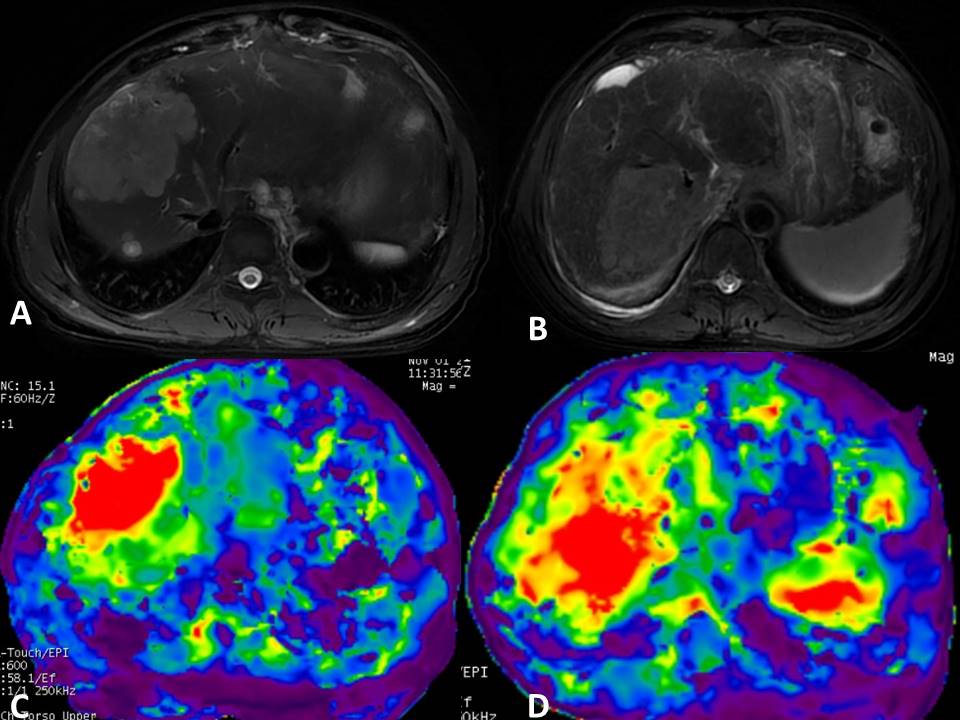
Fig.1 T2WI/FS and stiffness map of intrahepatic cholangiocarcinoma (A、C) and hepatocellular carcinoma (B、D), The measured values of the lesion stiffness were approximately 9.73kPa、11.46kPa. Liver background stiffness were approximately 4.66 kPa、5.23 kPa.