1991
3D contrast enhanced high definition, free-breathing Dixon imaging using radial stack of stars and respiratory gating and tracking: Clinical comparison to state of the art breath hold Dixon imaging1Philips Healthcare, Best, Netherlands, 2Philips Healthcare, Switzerland, 3Institute for Radiology and Nuclearmedicine, Kantonsspital Winterthur, Switzerland
Synopsis
We investigated a motion immune Dixon TFE approach incorporating a 3D radial stack-of-stars acquisition module interleaved with a spiral excitation navigator to gate and track the acquisition. Image quality, sharpness and streaking artifact level and its variability over different patient breathing patterns is efficiently improved to an extent where it is preferred over the state-of-the art breath hold (BH) Dixon scans. Next to that, it allowed scan time reductions of 30% in average. This technique provides motion-free, high resolution hepatic imaging with the benefits of Dixon providing consistent good fat suppression over a large FOV with water, fat, IP and OP diagnostic information all-in-one scan.
Introduction
3D Dixon radial stack-of-stars [1] is a very promising method. Next to an all-in-one method that provides water, fat, IP and OP diagnostic information also in difficult inhomogeneous regions, it provides motion immunity without enforcing breath holds (BH). For T1 contrast enhanced body MRI these ingredients are essential since breath holding is typically an issue during contrast administration with the average patient group. Although inherently motion robust, radial sequences rely on a regular and shallow breathing pattern. This is especially important in Dixon methods where fat streaking and blurring can introduce non-diagnostic images. In this study, we investigate respiratory gating and tracking of the imaging volume to improve both streaking and blurring.
Methods
All examinations were performed on 1.5 and 3T clinical scanners (Ingenia, Philips Healthcare) with a torso coil. In a volunteer study of four subjects, the effects of respiratory gating, tracking, radial density and halfscan were validated. Hereby the radial Dixon acquisition module was interleaved with an optimized spiral excitation navigator acquisition [2] to gate and track the imaging volume. The optimized radial sequence then was investigated in 12 patients. Two sequences were compared: Sequence 1. Conventional BH 3D Dixon Cartesian, Sequence 2. 3D gated radial stack-of-stars Dixon. Sequence parameters of these sequences are:
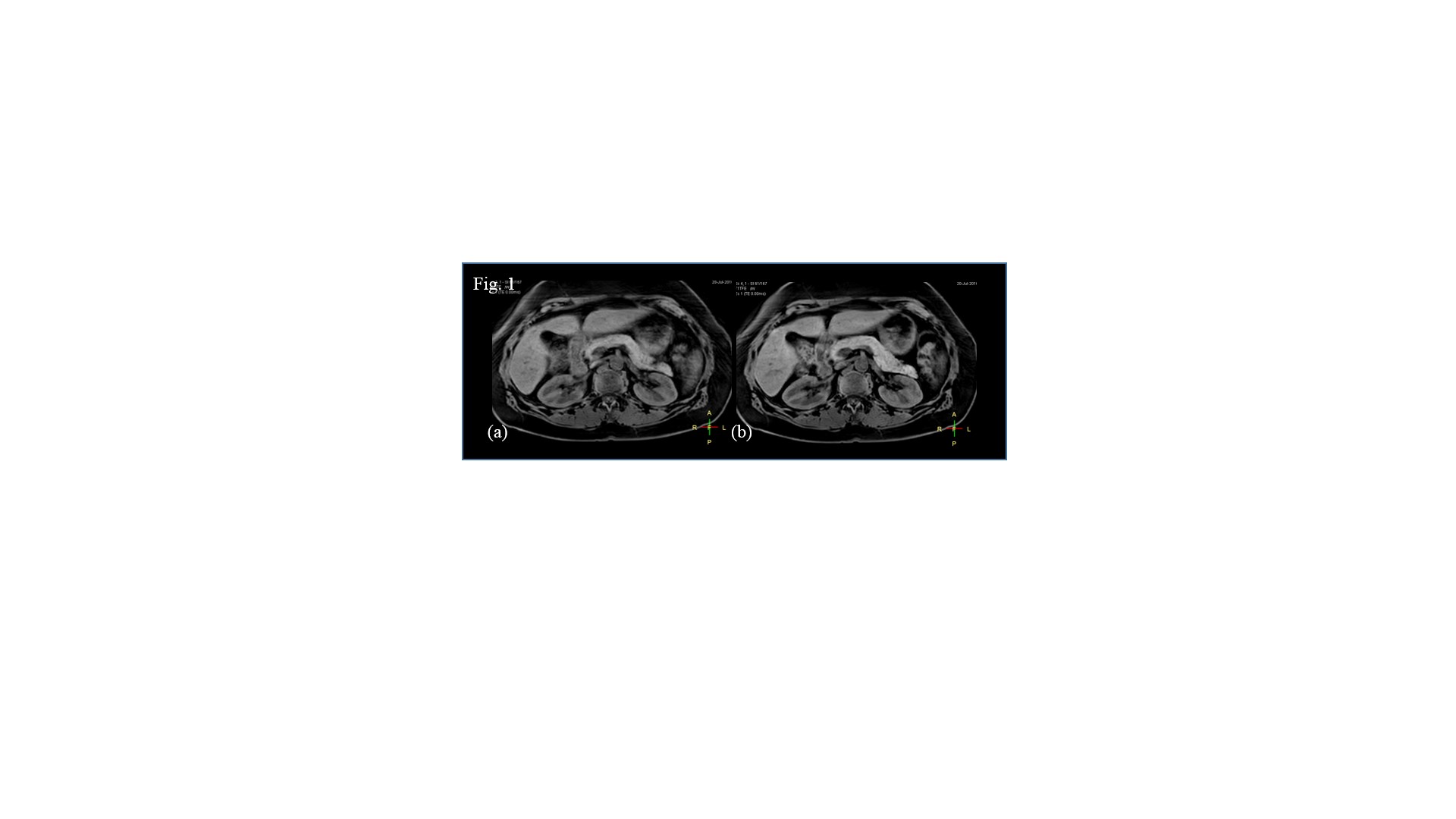
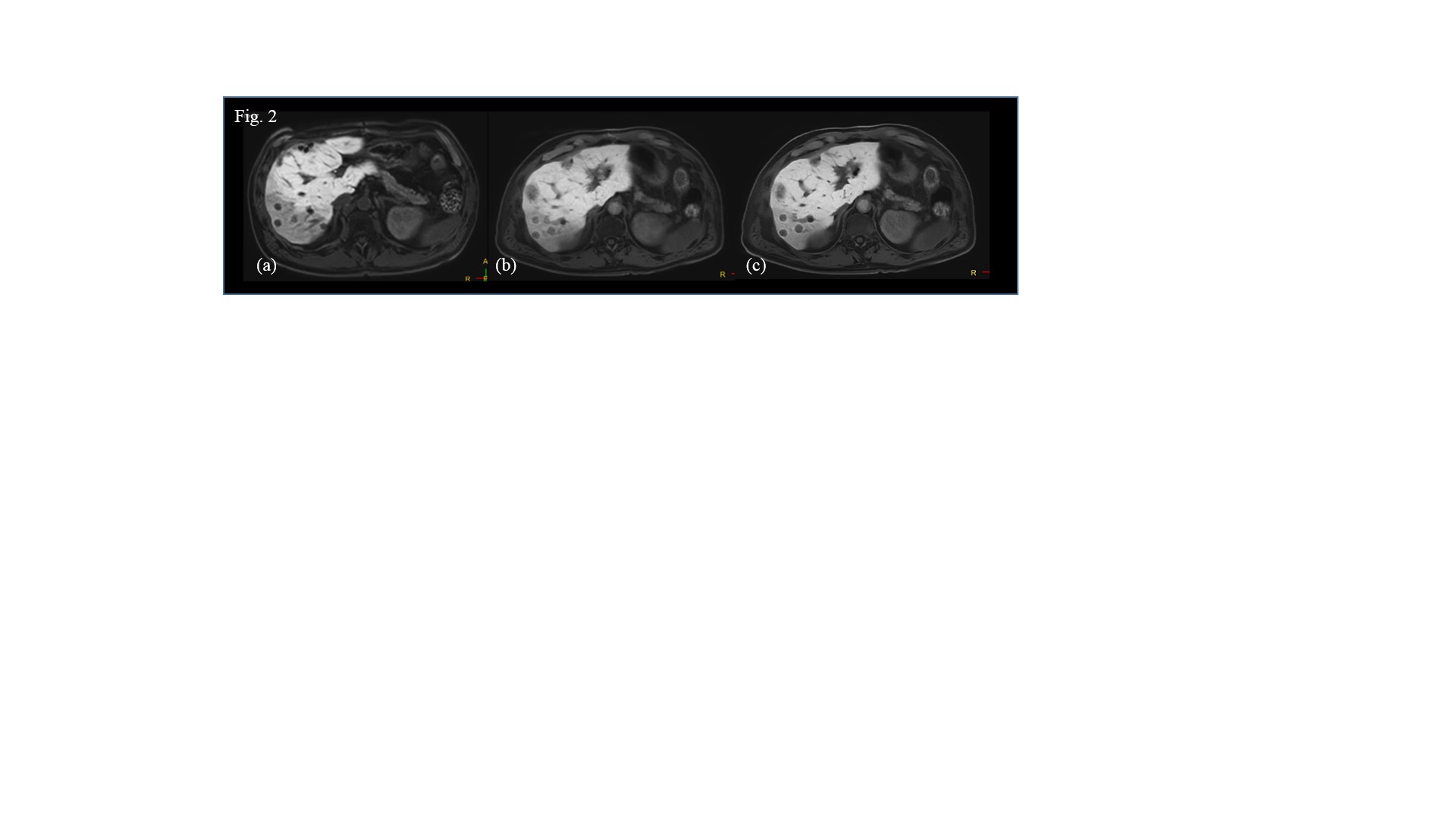
Sequence 1: 3D TFE, FOV = 400 x 352 mm2, resolution = 2.0 x 2.0 x 4.0 mm3, bandwidth = 555 Hz / pixel, flip angle = 15°, TR = 5.9 ms, TE 1 / TE 2 = 1.6 ms / 3.6 ms. SENSE Y, Z = 2.0, 1.3, halfscan Y, Z = 0.7, 0.85 leading to a scan time of 17 seconds.
Sequence 2: 3D radial TFE with Navigator gating (gating window= 10 mm), FOV = 450 x 450 mm2, resolution = 1.5 x 1.5 x 3.0 mm3, bandwidth = 1086 Hz / pixel, flip angle = 10°, TR = 4.7 ms, TE 1 / TE 2 = 1.4 ms / 2.6 ms, golden angle radial ordering, radial density = 200 %, SENSE Y, Z = 1.0, 1.8, halfscan Y, Z = 1.0, 0.7 leading to scan time of 2:40 minutes.
Overall image quality and sharpness were compared by reviews performed by two radiologists.
Results
In the volunteer study on four subjects, respiratory gating improved the image quality and its variability over different breathers showing reduced streaking artifacts and improved sharpness and contrast of the images. A respiratory gating window of 10 mm provided the most optimal setting effectively excluding breathing outliers and allowing to reduce the scan time by minimizing the radial percentage and halfscan factors. As a consequence the average scan time could be reduced by 30% in the respiratory gated scan compared to the non-gated radial stack-of-stars. Respiratory volume tracking furthermore improved the sharpness of the tracked organ of interest nevertheless at the cost of a potential increase in streaking and blurring of regions outside of the tracked volume. Hence in the patient study only respiratory gating was used. In the patient study, the respiratory gated radial stack-of-stars scan was preferred in 87.5 (+/- 4.5) % by the two independent reviewers compared to the conventional BH 3D Dixon scans (12.5 (+/- 4.5) %. In all cases, this was due to improved sharpness.
Discussion / Conclusion
We have demonstrated, that respiratory gating improves image quality (sharpness and streaking artifact level) and its variability over different patient breathing patterns to an extent where it is preferred over the state-of-the art BH Dixon scans. Next to that, it allows to drastically reduce acquisition time – in our case by 30% in average. This technique provides motion-free, high resolution hepatic imaging with the benefits of Dixon providing consistent good fat suppression over a large FOV with water, fat, IP and OP diagnostic information all-in-one scan.
Acknowledgements
No acknowledgement found.References
[1] Wuelbern et. al., ISMRM (2015), #3648
[2] Sachs et al., MRM 1994, vol 32, p. 639
Figures