1867
Age Related Diffusion and Tractography Changes in Typically Developing Pediatric Cervical and Thoracic Spinal Cord1Temple University, Philadelphia, PA, United States, 2Drexel University, Philadelphia, PA, United States, 3Radiology, Thomas Jefferson Hospital University, Philadelphia, PA, United States, 4Occupational Therapy, Thomas Jefferson Hospital University, Philadelphia, PA, United States, 5Radiology, Temple University, Philadelphia, PA, United States
Synopsis
This study investigates age related changes in diffusion tensor imaging and tractography parameters in pediatric spinal cord. This will help to understand maturation process in pediatric population and consequently will help for detection of diseased or injured spinal cord.
Introduction
Diffusion tensor imaging (DTI) and diffusion tensor tractography (DTT) has been shown to measure white matter integrity of spinal cord [1,2]. Recently DTI indices has been shown to change with age (ref) The purpose of this study is (a) to evaluate the maturational states of the entire pediatric spinal cordusing DTI and DTT indices including fractional anisotropy (FA), apparent diffusion coefficient (ADC), mean length of white matter fiber tracts and tract density and (b) to analyze the DTI and DTT parameters along entire spinal cord as a function of spinal cord levels.Methods
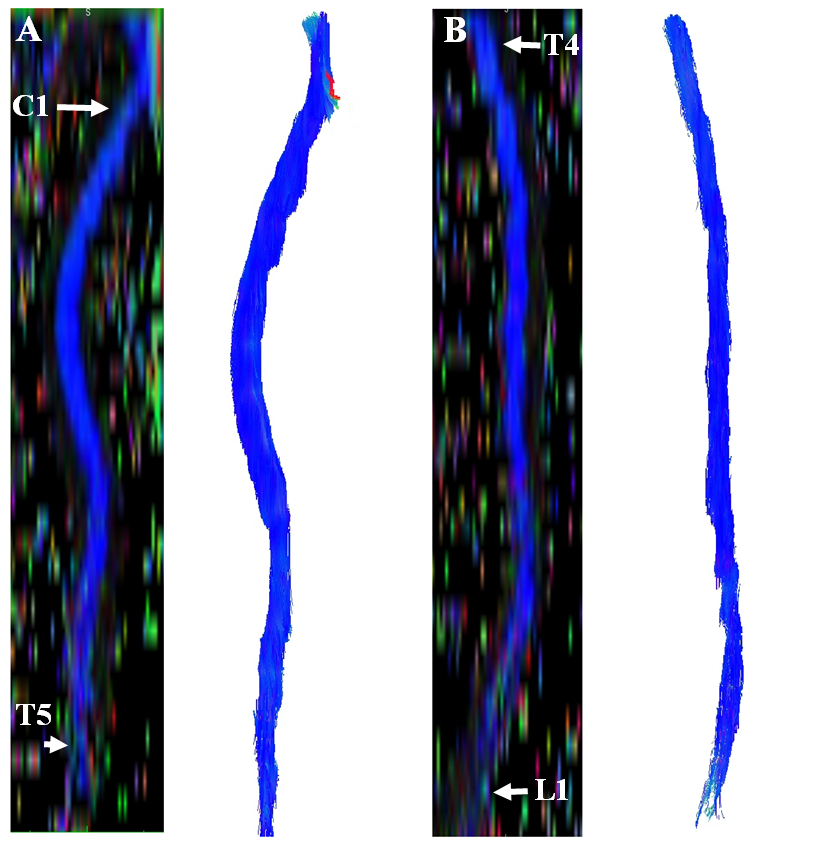
A total of 23 typically developing (TD) pediatric subjects ranging in age from 6-16 years old (11.94±3.26 (mean ±standard deviation)) were recruited, and scanned using 3.0T Siemens Verio MR scanner (Siemens Healthcare, Erlanger, Germany) with 4-channel neck matrix and 8-channel spine matrix coils. Reduced FOV diffusion tensor images were acquired axially in the same anatomical location prescribed for the T2-weighted images to cover the entire spinal cord (C1-mid L1 levels). The DTI parameters used were: FOV=164 mm, phase FOV=28.4% (47 mm), number of directions=20, b=800s/mm2, voxel size=0.8×0.8×6.0mm3, matrix size= 36×208, axial slices=40, TR=7900ms, TE=110ms, number of averages=3 and acquisition time=8:49min. Initially, diffusion directional images were aligned with the reference image (B0) using a rigid registration algorithm and a scaled least square cost function performed by in-house software developed in Matlab (MathWorks, Natick, Massachusetts) [1,2]. After motion correction, diffusion tensor maps (FA and ADC) and streamline deterministic tractography were generated from DTI data (https://med.inria.fr/) (Figure 1) with the scan specific gradient table and image orientation information. DTI and DTT parameters were calculated by using ROIs drawn on the whole cord along the entire spinal cord being anatomically localized by an independent board certified neuroradiologist [2,3]. These indices then were compared between two age groups (age group A=6–11 years (n=11) and age group B=12–16 years (n =12)) based on similar standards and age definitions used for reporting spinal cord injury in the pediatric population [4]. Standard least squared linear regression model based on restricted maximum likelihood (REML) method (using JMP pro 13.0 software) was used to evaluate the relationship between age and DTI and DTT parameters.Results
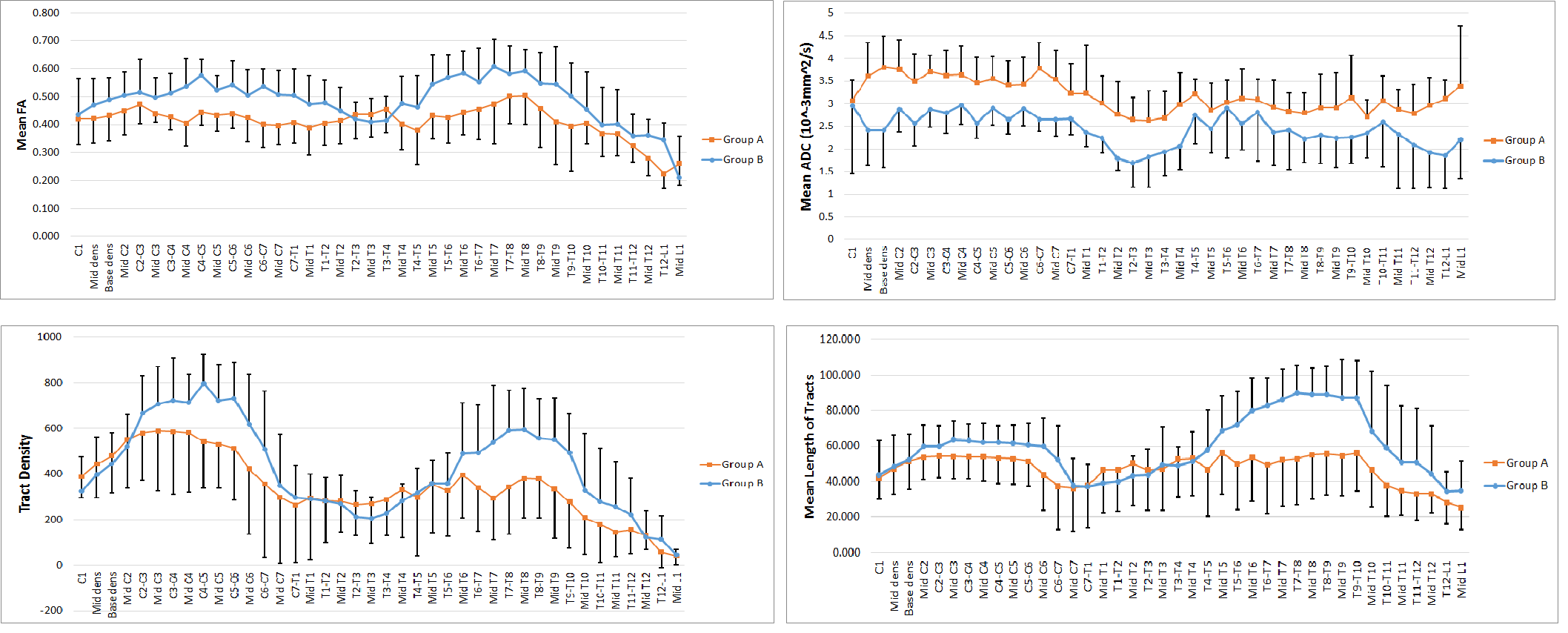
An increase in FA (group A=0.42±0.097, group B=0.49±0.116), white matter tract density (group A=368.01±236.88, group B=440.13±245.24) and mean length of fiber tracts (group A=48.16±20.48mm, group B=61.56±35.65mm) and a decrease in ADC (group A=3.19±0.69×10-3mm2/sec, group B=2.45±0.73×10-3mm2/sec) were observed with age along the entire spinal cord. Statistically, significant increases have been shown in FA (p=0.016), tract density (p<0.0001), mean length of fiber tracts (p=0.0004) and significant decrease has been shown in ADC (p=0.0078) between group A and group B. Also, it has been shown DTI and DTT parameters vary along spinal cord as a function of spinal cord level (Figure 2).Discussion
This study provides an initial understanding of DTI values as well as DTT of the spinal cord. The results show significant differences in DTI and DTT parameters which may result from decreasing water content, myelination of fiber tracts, and the thickening diameter of fiber tracts during maturation process.Conclusion
In conclusion, when quantitative DTI and DTT of the spinal cord is undertaken in pediatric population; an age and level matched normative data should be used to accurately interpret the quantitative results.Support:
This work was supported by National Institute of Neurological Disorders of the National Institutes of Health under award number R01NS079635.Acknowledgements
No acknowledgement found.References
[1] Izlem Izbudak, Netsiri Dumrongpisutikul, Carol B Thompson, Aylin Tekes, Majda Thurnher and Thierry AGM Huisman. Diffusion Tensor Scalars Vary with Age and Across Spinal Levels in Children, jneuro, 2015; 6(4): 1-6.
[2] Chris J. Conklin, Devon M. Middleton, Mahdi Alizadeh and et al. Spatially selective 2D RF inner field of view (iFOV) diffusion kurtosis imaging (DKI) of the pediatric spinal cord, NeuroImage: Clinical 11 (2016) 61–67.
[3] Mahdi Alizadeh, Alani Intintolo, Devon Middelton, Chris Conklin, Scott Faro, MJ Mulcahey, Feroze Mohamed. Reduced FOV Diffusion Tensor MR Imaging and Fiber Tractography of the Pediatric Cervical Spinal Cord. Spinal Cord Journal, spinal cord, 2016; 1-7.
[4] S. Saksena, D.M. Middleton, L. Krisa, P. Shah, S.H. Faro, R. Sinko, J. Gaughan, J. Finsterbusch, M.J. Mulcahey, and F.B. Mohamed. Diffusion Tensor Imaging of the Normal Cervical and Thoracic Pediatric Spinal Cord, 2016; 37(9): 1-8.
Figures