1861
Diffusion Entropy of Fractional Anisotropy Values in White Matter in Mild Traumatic Brain Injury1Pediatrics, University of British Columbia, Vancouver, BC, Canada, 2University of British Columbia, Vancouver, BC, Canada, 3Radiology, University of British Columbia, Vancouver, BC, Canada, 4Division of Sports Medicine, University of British Columbia, Vancouver, BC, Canada
Synopsis
A paper in Radiology by Delic et al. in 2016 looked at the Shannon entropy of fractional anisotropy values in white matter in the brains of people with mTBI and controls, and found significant differences between the two. We attempted to replicate their findings with retrospective mTBI data of our own. We did not find any significant differences with controls, and ice hockey athletes concussed after two weeks. We also did not find any changes in concussed athletes comparing data before injury with data after 3 days, 2 weeks, and 2 months.
Introduction
Over the past several years, concussions (mild Traumatic Brain Injuries (mTBI)), were seen by and large as minor injuries[1]. This is partly due to the mild symptoms - headaches, dizziness, trouble concentrating - that recover in a short period of time, and absence of findings on conventional medical scans. However, with repeated mTBIs, more severe symptoms may arise, such as those similar to degenerative brain diseases such as Alzheimer’s disease or Parkinson’s disease in some professional athletes[1]. Thus, the application of advanced MRI imaging in this area has attracted much attention from research scientists and clinicians, attempting to visualize and measure white matter injuries not apparent on conventional clinical scans. An article in Radiology by Delic et al.[2] recently showed promise in showing differences in mTBI and controls using Shannon entropy (SE)[3] to calculate whole-brain fractional anisotropy complexity. One significant benefit to this method is the availability of a single value that represents whole-brain changes due to mild brain injury. Using previous data we collected in varsity hockey players and controls, we attempted to replicate Delic et al.'s findings.
Methods
Subjects: This study used data acquired from an earlier completed study, and is thus retrospective. Forty amateur ice hockey players (mean age ± SD) = 21.2±3.1years) from two Canadian Interuniversity Hockey teams participated in the study. All players were scanned (baseline) before the beginning of the hockey season (September). An independent physician was on hand for all games, in order to diagnose concussions. If a player was concussed, they were then scanned at 72hrs, 2weeks, and 2months after their concussion. Of the original 45 athletes, 11 sustained a concussion and were subsequently scanned. 15 non-varsity university controls were recruited with similar gender and age as the athletes.
MRI: MRI data were acquired on a Philips Achieva 3T scanner. All subjects underwent the following set of scans: sagittal 3D T1-weighted scan (TR/TE/flip angle=8.1ms/3.7ms/6°; acquisition matrix/FOV/acquired voxel size/reconstructed=256x256x160/256x256x160mm$$^3$$/1x1x1mm3/1x1x1mm3); and DTI scan (TR/TE/flip angle=7015ms/60ms/90°; acquisition matrix/FOV/acquired voxel size/reconstructed/slice thickness=100x99/224x224mm2/2.2x2.2mm2/2x2mm2/2.2mm; b0=0, b1=700sec/mm2, 60 non-collinear directions).
Data Processing: DTI data was eddy current corrected, brain extracted, and FA values calculated using FSL. White matter masks were created using FSL FIRST. Shannon entropy (SE) values were calculated from the WM FA masks using Equation (1)[3] (in-house written software (MATLAB)). For each subject, a WM FA histogram was created using 197 bins [2]. Probability density functions for each bin were calculated. Substituting these values into Equation (1) gave the SE value.
Equation(1): $$ SE(x_i)=-\sum_{x_{i} \epsilon k} {(p(x_i)log(p(x_i))}$$
Statistics: A linear mixed effects model (LMEM) was used to compare SE means across controls (n=15), non-concussed athletes pre-season (n=40), and concussed athletes at two-weeks post-concussion (n=10). Sex and age were used as fixed effects, with intercepts for category as random effects. Two weeks was chosen as the timeline to compare as this is where we had most concussed data, and it is closest to the median in the Delic study [1]. LMEL was also used to analyze the relationship between mean SE values over time in concussed athletes (n=11 at baseline, n=8 at 72hrs, n=10 at 2wks, and n=9 at 2mnths). Time was used as a fixed effect, with intercepts for subjects as random effects.
Results
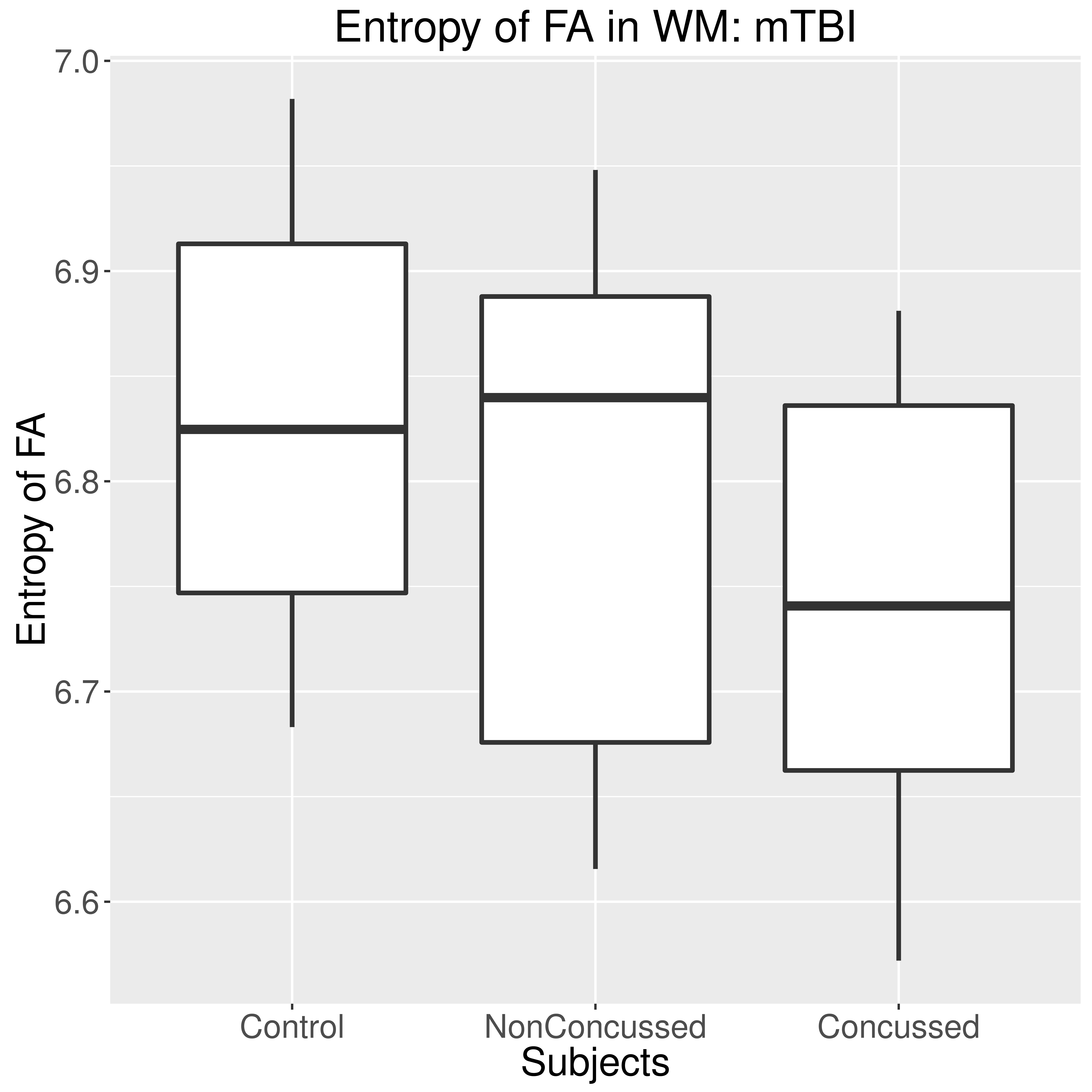
Figure 1 is a boxplot showing the SE of FA of WM in control subjects (n=15), non-concussed Hockey players at baseline (n=29), and concussed hockey players after 2 Weeks post-concussion (n=10). No significant differences were found.
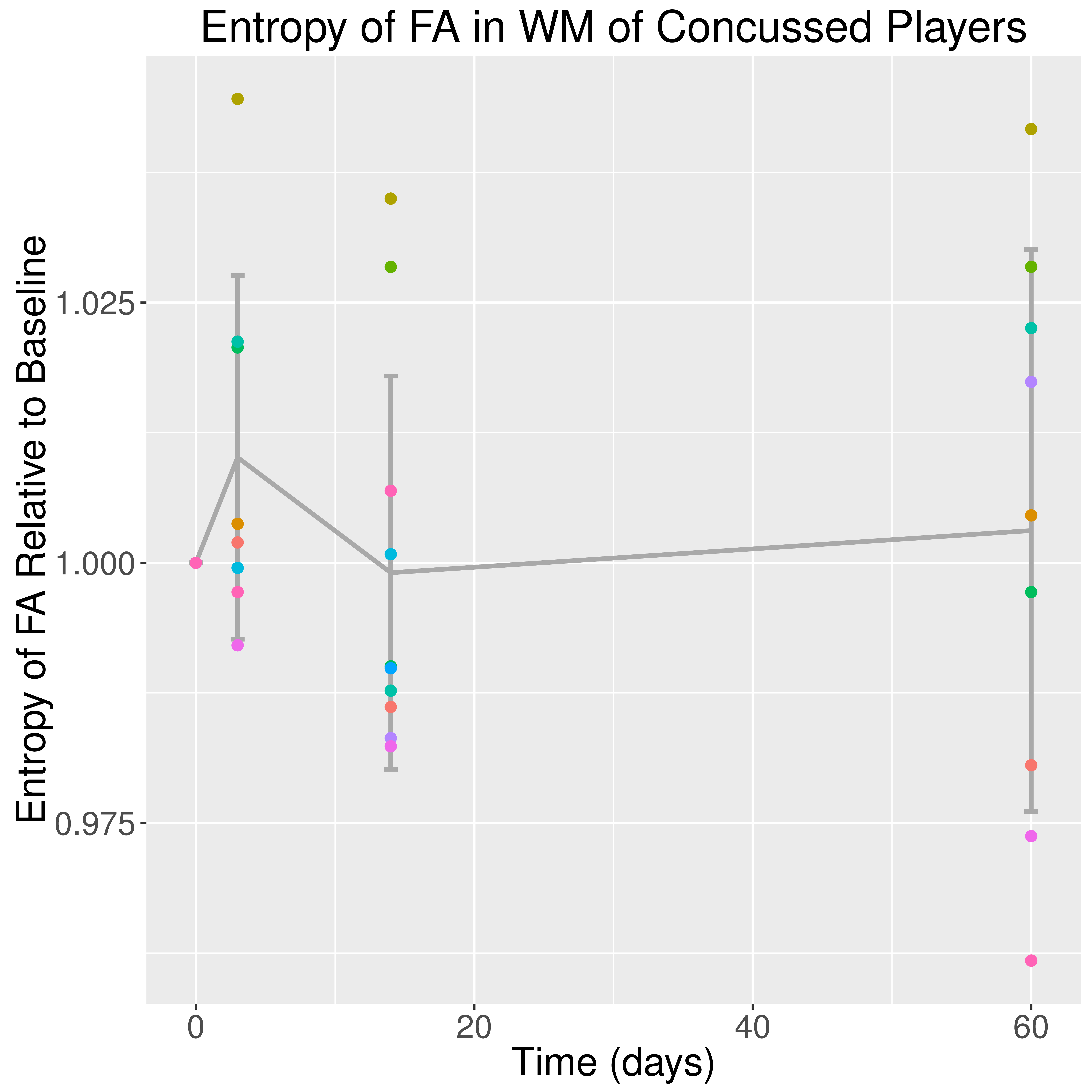
Figure 2 shows the longitudinal plot of SE of FA for athletes who received a concussion. A linear mixed effects model did not show any significant changes over time.
Discussion
Unlike Delic et al.[2], we did not find any differences in SE of WM FA in subjects with mTBI compared to controls. As well, we looked at subjects who sustained a concussion longitudinally, including data before injury. No significant changes were observed in SE of FA of WM over time.
This is the first known attempt to replicate these findings. We must consider several reasons that we did not see the same result as Delic et al.: their study had 74 mTBI subjects, much more than our 11, with a greater range in age; time of imaging post-concussion ranged from 0-506 days compared to our use of data after 14 days; 57% of mTBI injuries were sports related compared to our 100%; inclusion of PTM, and more.
Ultimately the usefulness of the SE of WM FA metric remains uncertain. As there are many studies that have looked at DTI in concussion, more retrospective analyses of these datasets are possible and recommended.
Acknowledgements
Author contributions: A.R., J.T. and D.L. designed the study. A.R. and D.L. designed the imaging protocol. S.D. collected data and helped coordinate the study. M.J., and A.M.W. performed data analysis under the supervision of A.R. A.M.W. wrote the abstract.
Competing interests: The authors declare that they have no competing interests.
Data and materials availability: Data is available and may be provided under the transfer policies of UBC. Funding: This research was funded by a London Drugs Award for Research Excellence in Radiology and a New Investigator Award to A.R. from the Canadian Institute for Health Research. A.R. is now supported through a Canada Research Chair. A.M.W. is supported by a Child and Family Research Institute – M.I.N.D. Postdoctoral Fellowship.
References
1. Canadian Institute for Health Information (CIHI). Head Injuries in Canada: A Decade of Change (1994-1995 to 2003-2004) [Internet]. 2006 [cited 2016 Apr 8]. Available from: https://secure.cihi.ca/estore/productFamily.htm?pf=PFC1360&lang=en&media=0
2. Delic J, Alhilali LM, Hughes MA, Gumus S, Fakhran S. White Matter Injuries in Mild Traumatic Brain Injury and Posttraumatic Migraines: Diffusion Entropy Analysis. Radiology. 2016 Jun;279(3):859–66.
3. Shannon CE. A mathematical theory of communication. Bell Syst Tech J. 1948 Jul;27(3):379–423.
Figures