1860
The diffusion kurtosis imaging findings of preoperative glioma-related epilepsy1The First Affiliated Hospital of Zhengzhou University, Zheng Zhou, People's Republic of China, 2The First Affiliated Hospital of Zhengzhou University, 3MR Scientific Marketing Specialist, Siemens Healthcare Ltd.,Shanghai,201318, China
Synopsis
MK not only reflects the microstructure of the glioma, but also may reflect neurotransmitter metabolism microenvironment.
Background
Patients with temporal, insular and frontal gliomas are more likely to experience seizures, and low-grade gliomas with oligodendroglial histology are strongly associated with preoperative seizures[1].There are many other strong risk factors for glioma-related epilepsy that have been highlighted in previous research, including high levels of glutamate and adenosine kinase and low levels of gamma-aminobutryic acid[2-3].Purpose
The aim of this study was to evaluate the difference of diffusion kurtosis imaging (DKI) parameters in the classification of preoperative glioma-related epilepsy.Materials and Methods
The institutional review board approved this prospective study, and informed consent was obtained from all patients. Every patient under resting state underwent diffusion kurtosis imaging (541s) and conventional sequence at 3.0 T MR scanner (Prisima Siemens Healthcare, Erlangen, Germany). 64 channel of head-neck coil was used for signal reception. DK imaging acquires data with six b values (0, 500,1000, 1500, 2000, and 2500 sec/mm2) and uses diffusion encoding in 30 directions for every b value. DKI was scanned using a spin-echo echo-planar imaging sequence and the parameters were: FOV = 220×220 mm2, slice thickness = 5 mm, slices = 20, TR/TE = 3500/78 ms. DKE post-processing software was used to calculated diffusion parameters—fractional anisotropy (FA), mean kurtosis (MK), and radial kurtosis (RK) and axial kurtosis (AK)—were calculated in the solid part of glioma. Regions of interest (ROIs) were manually drawn around the solid part of the tumor. According to the result of Kolmogorov–Smirnov (K–S) test, Independent-samples T test or Mann-Whitney-Wilcoxon test was used. A value of P < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS statistics software (version 21.0, IBM).Results
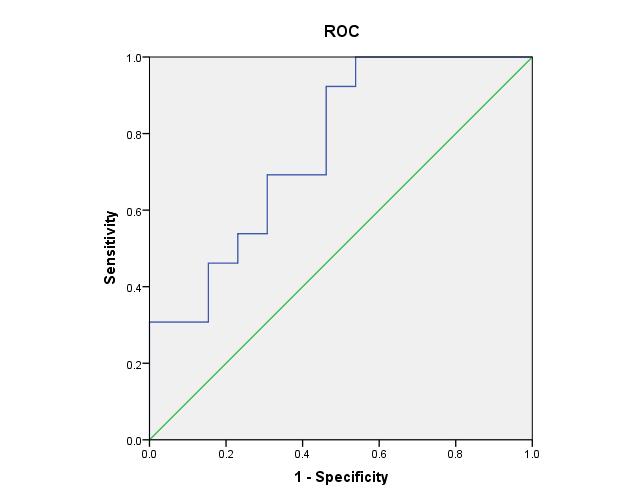
26 gliomas were observed, 13 patients with simplex partial epilepsy and 13 with generalized tonic-clonic epilepsy, and the pathologic diagnosis of them include 10 high-grade gliomas and 16 low-grade gliomas. 14 of them located at left cerebral hemisphere and the other 12 at right. The average longest diameter of them was 45.6mm. The tumors tend to spanned multiple lobes, include the frontal (n=17), parietal (n=5), insular (n=5) and temporal (n=11) lobes. There is no significant differences between high and low grade glioma groups on the basis of FA, MK, RK and AK (P>0.05). However, MK is significant higher in simplex partial epilepsy group [(1.032±0.21) × 10-3 mm2/s, MD ± SD] than that in generalized tonic-clonic epilepsy group [(0.718±0.21) × 10-3 mm2/s,MD ± SD, P = 0.007]. Taking 0.737 × 10-3 mm2/s as cut-off value for classified simplex partial epilepsy and tonic-clonic epilepsy, the sensitibity was 92.3% and specificity was 53.8%, and the AUC is 0.763.Conclusion
DKI parameters may be useful for the classification of preoperative glioma-related epilepsy.Discussion
MK not only reflects the microstructure of the glioma[4], but also may reflect neurotransmitter metabolism microenvironment.Acknowledgements
No acknowledgement found.References
[1]de Robles P, Fiest KM, Frolkis AD, et al. The worldwide incidence and prevalence of primary brain tumors: a systematic review and meta-analysis. Neuro Oncol 2014. Oct 13. pii: nou283
[2] Berntsson SG, Malmer B, Bondy ML. Tumor-associated epilepsy and glioma: are there common genetic pathways? Acta Oncol 2009;48:955963.
[3] Labrakakis C, Patt S, Hartmann J, et al. Functional GABA(A) receptors on human glioma cells. Eur J Neurosci 1998;10:231–8.
[4] Raab P, Hattingen E,Franz K,et al. Cerebral gliomas: diffusional kurtosis imaging analysis of microstural differences. Radiology. 2010;254(3):876-881.Figures
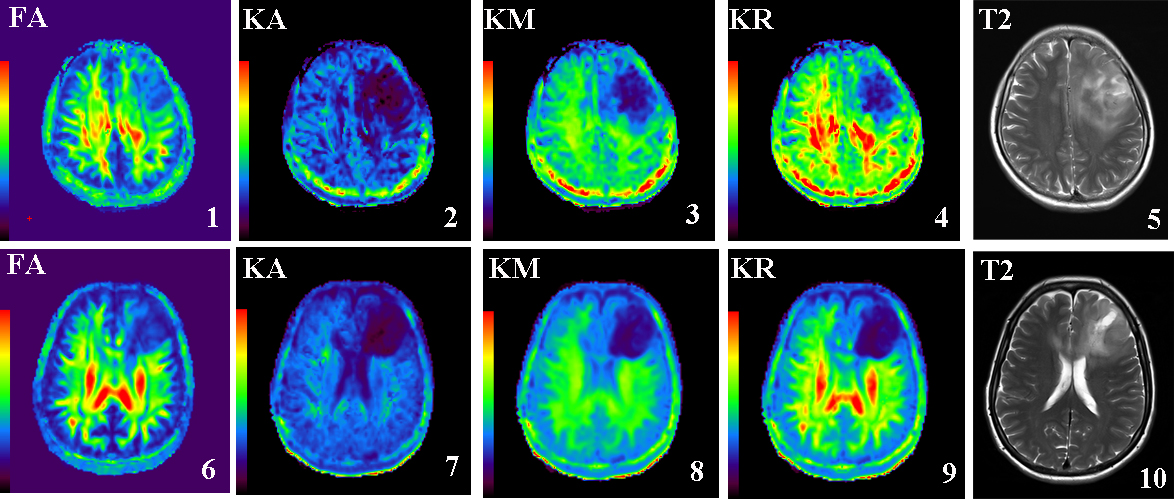
Picture1-5 is DKI parameter for 37years old, femal, oligodendroglioma,WHO 2 grade,tonic-clonic epilepsy.
Picture6-10 is DKI parameter for 48years old, femal, oligodendroglioma,WHO 2 grade,simplex partial epilepsy.