1713
Effects of Lithium on resting-state fMRI in HIV-associated neurocognitive disorder1Department of Electrical and Computer Engineering, University of Rochester, Rochester, NY, United States, 2Department of Imaging Sciences, University of Rochester Medical Center, Rochester, NY, United States, 3Department of Medicine, Stellenbosch University, South Africa, 4Department of Medicine, University of Cape Town, South Africa, 5Department of Psychiatry and Mental Health, University of Cape Town, South Africa, 6Department of Neurology, University of Rochester Medical Center, Rochester, NY, United States
Synopsis
This study firstly tested adjunctive lithium therapy in HIV patients with HAND. We examined the lithium effect using resting-state fMRI, and functional connectivity, amplitude of low-frequency fluctuation(ALFF) and fractional ALFF were calculated. We found significantly decrease of low-frequency oscillation and functional connectivity in lithium-treated group compared to placebo group, while neurocognitive performance was not different between the two groups.
Purpose
Lithium may be neuroprotective[1] and in pilot studies, has been reported to improve neurocognitive performance, increase fractional anisotropy, as well as affect brain activation patterns in HIV infected individuals[2-4]. Furthermore, lithium may also increase grey matter volume[5]. Here, we report the results of the effect of lithium on amplitude of low-frequency fluctuation (ALFF), fractional ALFF (fALFF)[6,7], and functional connectivity (FC).Methods
The study is the first test of adjunctive lithium therapy in HIV patients with moderate to severe HIV-associated neurocognitive disorder (HAND)[8] in a randomized double blind controlled trial. 61 HIV-infected adults were enrolled and completed in this study, all with Global Deficit Score (GDS)≥0.5 used as a measure of cognitive performance. All subjects were on combination antiretroviral therapy (cART) for at least 6 months with a suppressed viral load. Of the 61 enrolled, 44 had completed rs-fMRI data, 24 of them were lithium-treated, and the other 20 were on placebo.
Both groups were scanned before and after lithium/placebo treatment. The mean interval of two MRI scans was 212±24 days. MRI was acquired on a 3T Siemens Allegra syngo MRI scanner with standard sequences. A T1-weighted MPRAGE (repetition time (TR)/inversion time(TI)=2530/1100 ms, echo time (TE)=1.53/3.21/4.89/6.57 ms, voxel size=1.3x1x1.3 mm3, flip angle=7°, bandwidth=651 Hz/pixel) was acquired. Resting-state functional MRI was acquired using an EPI sequence (TR/TE=2000/30 ms, flip angle=77°, voxel size=3.4x3.4x4 mm3; matrix size=64x64, 33 axial slices, volumes=238).
The preprocessing includes: removal of the first ten volumes, slice timing correction, motion correction, spatial smoothing using a FWHM=4mm Gaussian kernel, and band-pass filtered (0.01Hz-0.08Hz) to reduce the low-frequency drift and to exclude physiological noise. Preprocessing was performed using Data Processing Assistant for Resting-State fMRI (DPARSF)[9]. ALFF, fALFF, and the FC were calculated using REST v1.8[10]. Group ICA were calculated using Group ICA of fMRI Toolbox (GIFT, http://mialab.mrn.org/software/gift/index.html) to identify the Default Mode Network(DMN). The ALFF was calculated by converting each voxel’s time series to frequency domain using fast fourier transform, and the mean of square root of the power spectrum is defined as ALFF[6]. The fALFF is the ratio of power spectrum to that of the entire frequency range[7]. We calculated the voxel-based FC by correlating each voxel’s time series with the averaged time series within DMN. We also calculated ROI-based FC: each node in DMN was correlated with the other three nodes, and the ROI-based FC is the mean correlation of the 6 paired nodes. Statistical analysis was performed using SPM, REST, and R. We used paired t-test to compare before and after treatment for each group. We used two sample t-test to compare the lithium-treated group and placebo-treated group, while the before-treatment data were used as covariate to remove the inter-group variance.
Result
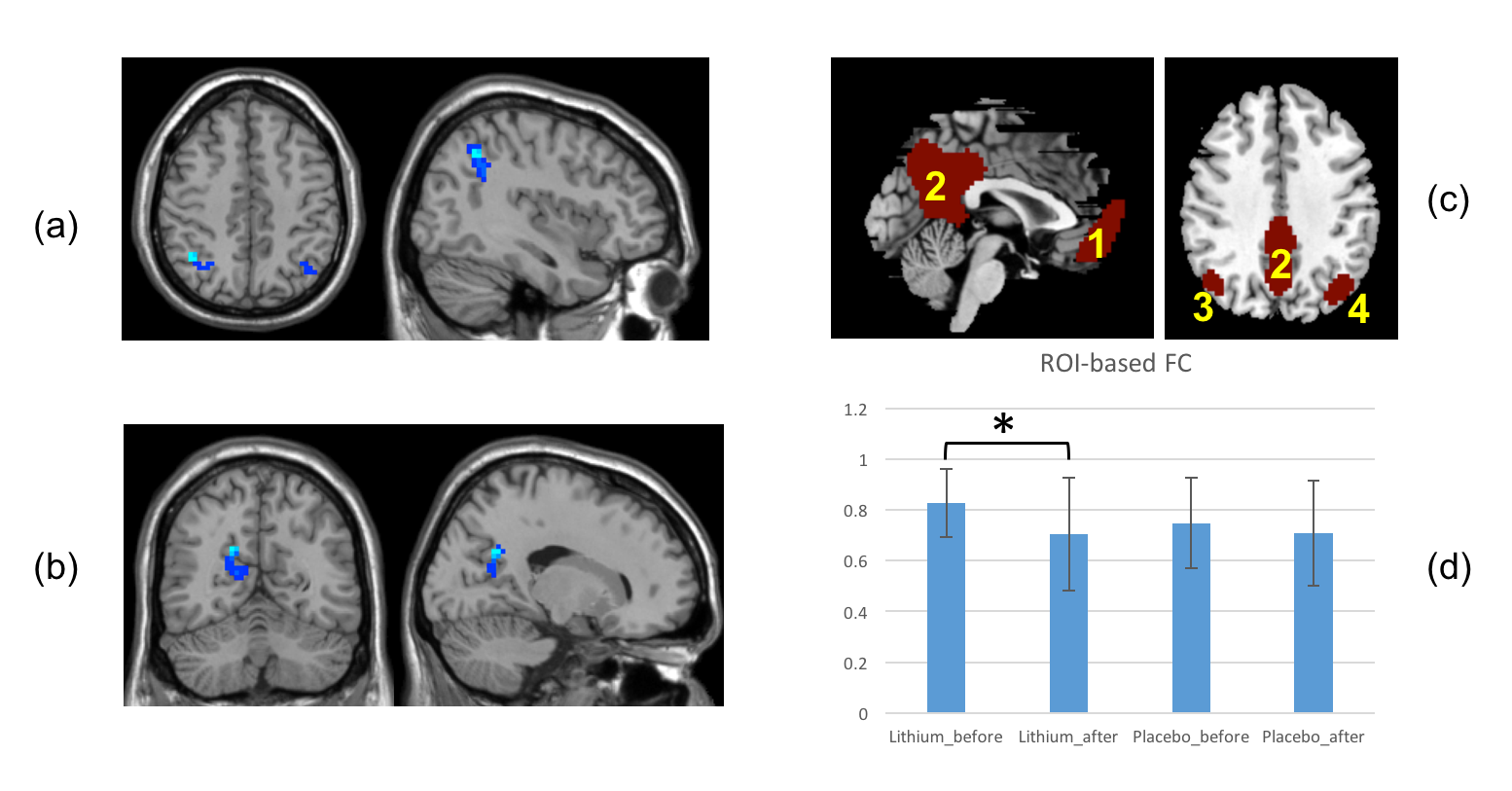
Both ALFF and fALFF showed significantly decrease in bilateral angular gyrus (Figure 1(a) AlphaSim correction, voxel p<0.01, cluster size>648mm3, correspond to a corrected p<0.05) in lithium-treated group compared to the placebo-treated group. At baseline, there was no significant difference between the two groups. The angular gyrus is considered as functional hubs in DMN. The voxel-wise FC showed significantly decrease in posterior cingulate gyrus after lithium treatment (Figure 1(b) AlphaSim correction, voxel p<0.01, cluster size>756mm3, correspond to a corrected p<0.05). The ROI-based within-DMN FC (Figure 1(c, d)) also showed significantly decrease after treatment compared to before treatment but only in lithium arm. We did not find significant correlations between changes in GDS and imaging metrics.Discussion
Our results show that lithium decreases brain activation, especially within DMN, in HIV infected individuals with cognitive impairment. The change in brain activation does not correlate with changes in cognitive performance. This raises the possibility that in the context of cognitive impairment, lithium has no benefit despite having a demonstrable effect on brain function. In previous studies of bipolar disorder, lithium was associated with reduced activation[11, 12] thus consistent with our results.Conclusion
Lithium reduces brain activation in patients on cART with HAND; however, this does not translate into additional benefit in terms of neurocognitive performance.Acknowledgements
No acknowledgement found.References
1. Dou, H., et al., Neuroprotective mechanisms of lithium in murine human immunodeficiency virus-1 encephalitis. J Neurosci, 2005. 25(37): p. 8375-85.
2. Tivarus, M.E., et al., Are Structural Changes Induced by Lithium in the HIV Brain Accompanied by Changes in Functional Connectivity? PLoS One, 2015. 10(10): p. e0139118.
3. Schifitto, G., et al., Lithium therapy for human immunodeficiency virus type 1-associated neurocognitive impairment. J Neurovirol, 2009. 15(2): p. 176-86.
4. Letendre, S.L., et al., Lithium improves HIV-associated neurocognitive impairment. AIDS, 2006. 20(14): p. 1885-8.
5. Hafeman, D.M., et al., Effects of medication on neuroimaging findings in bipolar disorder: an updated review. Bipolar Disord, 2012. 14(4): p. 375-410.
6. Zang, Y.F., et al., Altered baseline brain activity in children with ADHD revealed by resting-state functional MRI. Brain Dev, 2007. 29(2): p. 83-91.
7. Zou, Q.H., et al., An improved approach to detection of amplitude of low-frequency fluctuation (ALFF) for resting-state fMRI: fractional ALFF. J Neurosci Methods, 2008. 172(1): p. 137-41.
8. DECLOEDT, E.H., et al., Moderate to severe HIV associated neurocognitive impairment: a randomised placebo controlled trial of lithium. Medicine, 2016.
9. Chao-Gan, Y. and Z. Yu-Feng, DPARSF: A MATLAB Toolbox for "Pipeline" Data Analysis of Resting-State fMRI. Front Syst Neurosci, 2010. 4: p. 13.
10. Song, X.W., et al., REST: a toolkit for resting-state functional magnetic resonance imaging data processing. PLoS One, 2011. 6(9): p. e25031.
11. Silverstone, P.H., et al., Lithium alters brain activation in bipolar disorder in a task- and state-dependent manner: an fMRI study. Ann Gen Psychiatry, 2005. 4: p. 14.
12. Strakowski, S.M., et al., fMRI brain activation changes following treatment of a first bipolar manic episode. Bipolar Disord, 2016. 18(6): p. 490-501.
Figures