1708
Altered Functional Connectivity in Essential Tremor Patients immediately following Thalamotomy using MRI guided Focused Ultrasound1Center for Metabolic Imaging & Therapeutics, Department of Diagnostic Radiology & Nuclear Medicine, University of Maryland Baltimore School of Medicine, Baltimore, MD, United States, 2Department of Diagnostic Radiology & Nuclear Medicine, University of Maryland Baltimore School of Medicine, Baltimore, MD, United States
Synopsis
Essential tremor (ET) is a common neurological disorder. It is often characterized by progressive tremor of the arms or hands during voluntary movements. Ablation of the
Purpose
Essential tremor (ET) is a common neurological disorder with an estimated prevalence between 0.3% and 5.55%. It is often characterized by progressive tremor of the arms or hands that occurs during voluntary movements. Thalamotomy using magnetic resonance imaging guided high intensity focused ultrasound (MRgFUS) has been recently approved by the FDA and appears to be an effective treatment for ET where the ventralis intermedius nucleus (VIM) within the thalamus is targeted for ablation. However, little is known regarding changes in the brain networks among ET patients and even less regarding the changes in these networks following MRgFUS thalamotomy. Previous resting state functional MRI (rs-fMRI) studies have revealed that the disruption of functional connectivity (FC) in the cerebello-thalamo-motor cortical networks in ET patients1, 2. This study aims at investigating the changes in FC between the ablated VIM and the rest of the brain in ET patients immediately after the MRgFUS thalamotomy.Materials and Methods
Eighteen medication refractory ET patients (72.53 ± 5.10 years and 17M/1F, right-handed) were recruited to undergo thalamotomy using MRgFUS at the University of Maryland Medical Center. Each patient underwent thalamotomy of the left VIM. The degree of tremor was assessed using the Clinical Rating Scale for Tremors (CRST) before and after treatment. MRI scans were performed on a 3T Trio-Tim Siemens system before and 24 hours after treatment. The rs-fMRI data were acquired in the axial plane using T2* weighted single shot echo-planar imaging (EPI) technique with the following parameters (TR/TE: 3000/30 ms; flip angle 90o; spatial resolution 2.738 x 2.738 mm2; slice thickness 2.7 mm). A total of 200 volumes were acquired. High-resolution structural data was also obtained sagittal using 3D isotropic T1-MPRAGE sequence (TR/TE 2300/2.91 ms, Flip angle 9o, a spatial resolution of 1 x 1 x 1 mm3). The rs-fMRI data were preprocessed using SPM12 (http://www.fil.ion.ucl.as.uk/spm) including slice timing, realignment, normalized to the MNI template space, spatially smoothed with 6-mm full-width half-maximum (FWHM) Gaussian kernel, and temporally filtered with a bandpass filter of 0.008 Hz and 0.09 Hz. The T1-MPRAGE images were segmented into gray matter (GM), white matter (WM), and cerebral spinal fluid (CSF). The nuisance variables including the six motion correction parameters as well as the principle components of the WM and CSF mask were regressed out from the fMRI data to remove motion and non-neuronal contributions. Seed-based functional connectivity analysis was performed using the functional connectivity toolbox Conn (http://www.nitrc.org/projects/conn). The location of the left VIM (treated site) was estimated from the normalized T2 images after treatment and a 5 mm spherical ROI was placed on the left VIM. Functional connectivity difference map between pre- and post-treatment were created with thresholds at a voxel-wise uncorrected p-value of 0.005 and cluster-wise threshold p-value of 0.05 using FDR correction for multiple comparisons.Results
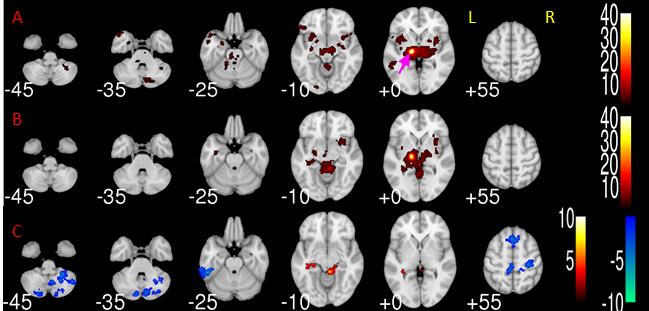
Significant alteration of functional connectivity between the left VIM and the rest of the brain are shown in the difference map of functional connectivity of Figure 1. Specifically, reduced functional connectivity between left VIM and cortical cortex after treatment was observed in the bilateral precentral, postcentral, superior frontal left inferior temporal gyri, as well as anterior and posterior cingulate cortices. Reduced functional connectivity between the left VIM and the cerebellum were found in bilateral cerebellar II and right cerebellar VI, VII, VIII, and IX. We also observed increased functional connectivity to the right cerebellar III, IV, V and left hippocampal gyrus.Discussion and Conclusion
Our findings reveal bilateral decrease in FC between the VIM and the motor and cerebellar cortices at 24 hours post-procedure. This decreased thalamo-motor-cerebellar connectivity is consistent with the observation that a significant number of patients (36%) exhibited gait disturbance at 24 hours post procedure with about 9% of the patients having continued gait disturbance at 12 months in the larger multi-center study which comprised of 76 patients3. Our results also demonstrate changes in FC in other non-motor areas including the left hippocampus, left temporal lobe, and superior frontal cortex suggesting the possibility of cognitive changes following the procedure. Overall these results suggest significant changes in both motor and non-motor networks immediately following the procedure. While most of the patients had sustained reduction in the tremor symptoms at 12 months, the long term effects of MRgFUS thalamotomy on neural networks remains to be examined. Future work will focus on the longitudinal changes in network connectivity of VIM thalamotomy using MRgFUS.Acknowledgements
No acknowledgement found.References
1. Julian Benito-Leon, Elan D. Louis et al. Altered functional connectivity in essential tremor a resting-state fMRI study. Medicine. 2015. 95: 49
2. Weidong Fang, et al. Essential tremor is associated with disruption of functional connectivity in the ventral intermediate nucleus-motor cortex – cerebellum circuit. Human Brain Mapping. 2016. 37: 165-178
3. Elias WJ, et al. A Randomized Trial of Focused Ultrasound Thalamotomy for Essential Tremor. N Engl J Med. 2016. 375(8):730-9.
Figures