1706
Resting state fMRI in MigraineKenneth M Jackson1, Steven C Liu1, Maryam Falahpour1, Christy Jackson2, Frank Haist3, Richard B Buxton1, and David J Dubowitz1
1Radiology, University of California San Diego, La Jolla, CA, United States, 2Neurology, Scripps Clinic, La Jolla, CA, United States, 3Psychiatry, University of California San Diego, La Jolla, CA, United States
Synopsis
We used resting state fMRI to evaluate changes in functional connectivity during migraine episodes, and the response to treatment. The results provide preliminary evidence for a change in functional connectivity in the DMN during migraine, and for the ability of serotonin agonists to restore resting state connectivity. We also identified key brain regions impacted by migraine and then normalized following sumatriptan.
Introduction
Migraine is a highly prevalent chronic condition characterized by a hyper-responsive nervous system that predisposes to recurrent episodes of severe headache and autonomic disturbance. In this study, we used resting state fMRI to evaluate changes in functional connectivity during migraine episodes, and the response to treatment with serotonin receptor agonist, sumatriptan. Key brain regions impacted by migraine and then normalized following sumatriptan were identified.Methods
5 female patients with ICHD-II diagnosis of menstrual migraine were recruited (patients were otherwise healthy with no additional cerebrovascular or neurological pathology). Resting state EPI data were acquired at 3 time points: (1) Baseline (during symptom-free luteal phase of menstrual cycle), (2) Migraine (during headache - typically day 1 of cycle), (3) Post treatment on same day, 2 hours following 6mg sc aerosol injection of sumatriptan (Sumavel DosePro). To control for variations in CBF and CMRO2 with menstrual cycle, 5 health female controls also underwent the same MR measurements at the same time points (and also received the sumatriptan injection). We acquired 334 EPI whole brain volumes (TR 1800ms, TE2 5ms, resolution 2.57 x 3.75 x 5mm, 10 minutes). AFNI, FSL and MATLAB were used for MRI data preprocessing. High-resolution anatomical images were bias field corrected and then skull stripped. Tissue segmentation was applied to estimate white matter (WM), cerebral spinal fluid (CSF) and Gray matter (GM) partial volume fractions. Functional data were then corrected for time-shift, motion, and physiological noise. Data was transformed to Talairach space and spatially smoothed (5mm FWHM). An anatomical parcellation of 116 cortical and subcortical regions (TT_caez_ml_18) was used to define ROI masks. The average BOLD time series was computed for each ROI. Temporal correlation between the ROIs were calculated and then normalized to Z-values for group analysis. Data were analyzed within the default-mode network (DNM), comparing changes in-group Z-score for patients vs. controls at each time point (baseline, migraine, Rx sumatriptan). To determine regions most impacted by the combination of migraine headache and serotonin injection, we created difference maps of migraine vs. baseline and sumatriptan vs. migraine and identified regions that showed a change in Z-score with migraine, and subsequently showed a reversal with sumatriptan. We used a Bonferroni correction, with a conservative alpha threshold of 0.00001 to allow for 5,000 repeated correlation measurements. Regions within these difference maps were ranked based on the number of other regions they were correlated with (above threshold). The top 10 regions whose interactions were most impacted by migraine and subsequently reversed by sumatriptan were identified.Results
Correlation maps for the 16 regions that defined DNM are shown in figure 1, with color scale showing the grouped z-score for the 3 timepoints: baseline, migraine, Rx sumatriptan. Figure 2 shows the change in mean Z-value with migraine and following sumatriptan treatment. There is a decrease in correlations (mean Z-score) in DMN during migraine headache, which is reversed with sumatriptan. Figure 3 shows the top ranked regions whose interactions were most impacted by the combination of migraine and subsequently reversed by sumatriptan. Total number of interactions above P<0.00001 threshold = 588. These top 10 regions accounted for 145 (25%) of these interactions.Discussion
The default mode network is most active during time of cognitive consolidation. Any intervention that disrupts this resting cognitive process would be expected to impact correlations within the network, thus we hypothesized that the psychological, physiological and autonomic changes that accompany migraine headache would be visible as a change in the network strength; and, furthermore, that treatment of the migraine headache would be expected to mitigate some of these disruptions in network correlations. A 2-way ANOVA did not detect a significant main effect of group (patient, control) or timing (baseline, migraine, sumatriptan). A one-tailed paired t-test comparing Z-score changes between migraine and baseline indicated that there is a trend (P=0.13), and additional subjects are needed to attain adequate power. However, the results provide preliminary evidence for a change in functional connectivity in the DMN during migraine, and for the ability of serotonin agonists to restore resting state connectivity. Our hypothesis focused on DMN, but our evaluation of addition regions impacted by migraine + sumatriptan indicate that additional functional networks may be more disrupted by migraine that DMN.Conclusions
These data provide preliminary evidence for a change in functional connectivity during migraine headaches. A functional network that includes regions in temporal and parietal cortex as well as subcortical regions in thalamus and cerebellum has been identified that appears to be active during the migraine headaches and responsive to serotonin agonists to restore resting connectivity.Acknowledgements
Supported by NIH R21 NS091709References
No reference found.Figures
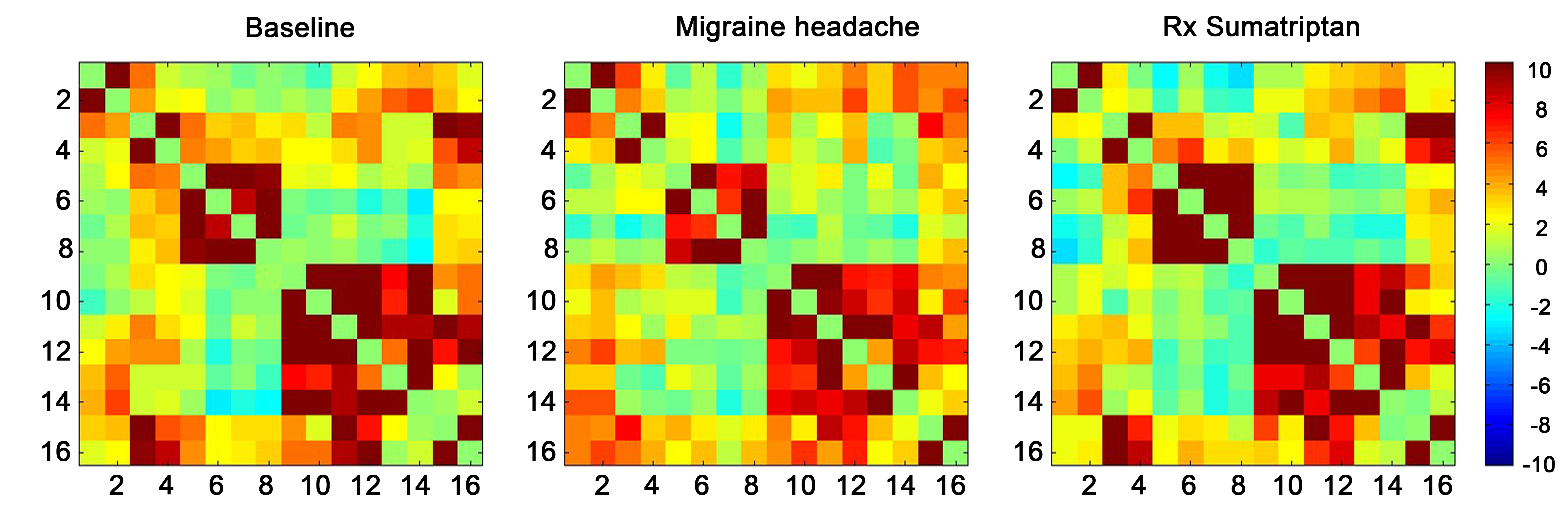
Correlation maps showing changes in DMN during migrain, and recovery
withy sumatriptan treatment. (The regions 1-16 are: left and right anterior
cingulate cortex, left and right
posterior cingulate cortex, left and right hippocampus, left and right
parahippocampal gyrus, left and right superior parietal lobule, left and right
inferior parietal lobule, left and right supramarginal gyrus, left and right
angular gyrus). Color scale is Z-score
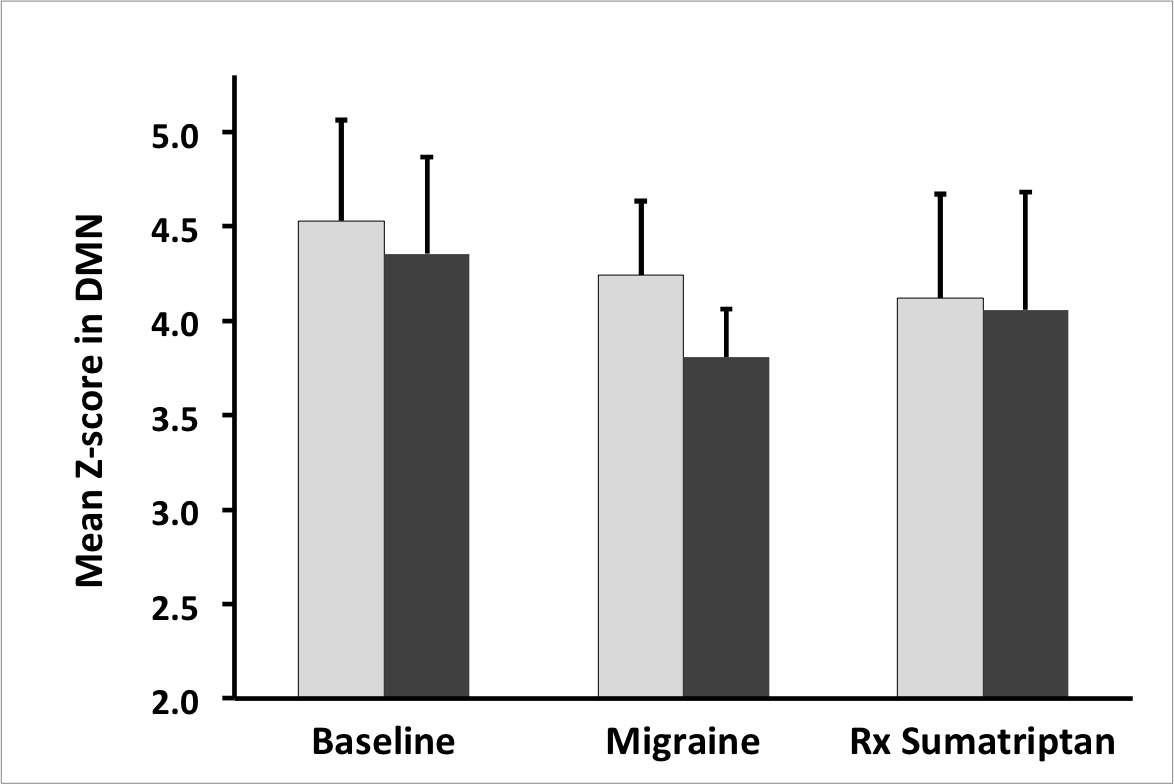
Mean correlation within DMN (expressed as a Z-score across the
group) shows decline in correlations with migraine and recovery with
sumatriptan.
(error bar = SE)
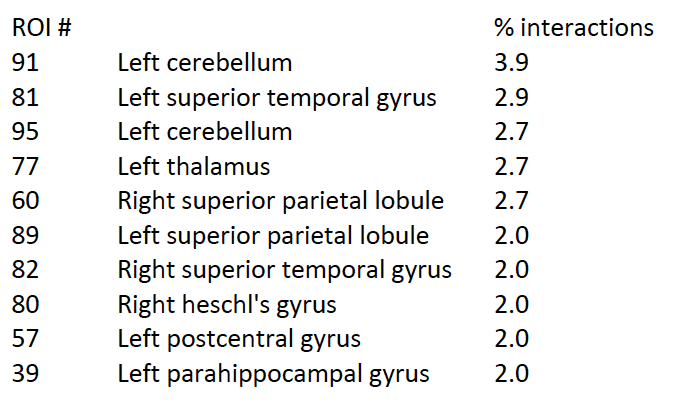
Top 10 ROI that define a network of regions whose interactions were
most impacted by migraine and subsequently reversed by sumatriptan. ROI number
is the index in the TT_caez_ml_18 parcelation map. % interaction shows the
contribution of each region to the total network defined by the response to
migraine and sumatriptan threatment.