1705
Resting state fMRI in Patients Infected with Hepatitis C VirusSantosh Kumar Yadav1, Ajay Vardaan2, Rakesh Kumar Gupta3, Pradeep Kumar Gupta3, Samir Mohindra4, Deepak Kaura5, Francesco Marincola1, Ena Wang1, and Mohammad Haris1
1Research Department, Sidra Medical and Research Center, Doha, Qatar, 2Department of Medicine, King George Medical University, Lucknow, India, 3Department of Radiology and Imaging, Fortis Memorial Research Institute, India, 4Department of Gastroenterology, Sanjay Gandhi Post graduate Institute of Medical Science, India, 5Department of Radiology, Sidra Medical and Research Center, Doha, Qatar
Synopsis
Current study measured the amplitude of low-frequency fluctuations (ALFF) and insular functional connectivity (FC) in Hepatitis C virus patients and compared with age and gender matched control using RESTplus software. HCV patients showed significantly reduced ALFF in the right insula. The right insular FC strength was lower in patients than control. Neuropsychological test scores were significantly lower in HCV patients. Changes in ALFF and FC provide new evidences of altered neuronal activity in HCV patients.
Introduction
Hepatitis C is a blood-borne disease caused by the hepatitis C virus (HCV). Around 3% of the world populations are living with the hepatitis C1. If untreated, it may cause liver cirrhosis subsequently hepatic encephalopathy (HE). HE is a potentially reversible neuropsychiatric disorder leading to cerebral edema induced by hyperammonia and inflammatory cytokines2. Neuroimaging studies have emphasized the structural and metabolic alterations in the brain of patients with hepatitis C3. In the current study, we investigated the altered spontaneous neuronal activity as measured by amplitude of low-frequency fluctuations (ALFF) and insular functional connectivity (FC) in these patients and compared with those of control.Materials and Methods
Institutional ethical committee approved the study protocol. With informed consent 9 HCV patient (mean age±sd, 38±13 years; 3 females/10 males), and 13 controls (mean age±sd, 33±12 years; 4 female/5 male) underwent for clinical examination, cognitive assessments and brain MRI. MRI was performed on a 3T clinical MR scanner (Signa HDxt, General electric, Milwaukee, USA). RS-fMRI data were acquired using an echo-planar imaging with following parameters: TR = 2.5 s, TE =30 ms, flip angle = 90°, number of slices = 46, slice thickness = 3 mm, and 120 volumes per acquisition together with higher resolution 3D-T1-weighted imaging were also performed. Data were processed using SPM8 (http://www.fil.ion.ucl.ac.uk/), and analysis were performed using RESTplus (http://restfmri.net/). The initial 10 volumes of the functional images were removed, and rest of the images were corrected for the slice timing and rigid bodymotion. High-resolution structural images were normalized to the MNI template using dartel and normalization parameters were applied to EPI images. Subjects with excessive head motion (displacement=3mm; angular rotation=3 degree) were excluded. Spatial smoothing was performed with an isotropic Gaussian kernel of 6mm of FWHM. The rs-fMRI data were temporally band-pass filtered (0.01-0.08 Hz) to reduce the very low frequency drift and high-frequency respiratory and cardiac noise. The time series for each voxel was transformed to the frequency domain and then the power spectrum was obtained. The square root was calculated at each frequency of the power spectrum. The averaged square root was taken as ALFF. For standardization, the ALFF of each voxel was divided by the global mean of ALFF values within a brain mask. For FC analysis, the seed ROI for right insula was generated as this region showed significantly decreased ALFF signal in patients. The mean time series of ROI was calculated by averaging the time series of all voxels within the ROI. Then a voxel-wise correlation analysis was performed between the mean time series of ROI and the time series of the remaining brain areas. Finally, Fisher’s z-transform was applied to improve the normality of the correlation coefficients. Head motion, CSF volume, white matter signal and global mean signal were used as covariates in the analysis.Statistical Analysis
Demographic and cognitive profiles were assessed by independent samples t-tests and Chi square. A two-sample t-test was performed to evaluate the ALFF difference between the HCV patients and controls. For FC analysis from a seed ROI (right insula) within each group, one sample t-test was performed in a voxel-wise manner to determine the regions with significant positive connectivity to the whole brain. A threshold of p< 0.001 with a minimum cluster size of 165 voxels was used to correct for multiple comparisons using AlphaSim along with age and gender as covariates.Results and Discussion
No significant differences were observed either in gender (p = 0.6) or age (p = 0.32) between groups. Compared to controls, HCV patients showed significantly decreased ALFF in the right insula (figure 1 A, B). Right insular FC associated positively with the multiple brain sites both in control and patient (figure 1 C, D). However, in HCV patients the FC strength was lower than the control. Neuropsychological test scores were significantly lower in HCV patients than control (data not shown). There are evidences from neuroimaging studies linking the insular area to cognitive and nonmotor functions4,5. Decreased ALFF in the right insula may relate to the cognitive impairments in these patients as insular area play key role in regulating various brain networks, which was further supported by the reduced FC of right insula to the other brain regions in HCV patients.Conclusion
Changes in ALFF and FC in the right insula provide new evidences of altered neuronal activity in HCV patients. The current findings further provide insight into the biological mechanism of the disease.Acknowledgements
Sidra Medical and Research Center provides the work station to process the MRI data.References
(1). Averhoff FM, Glass N, Holtzman D. Global burden of hepatitis C: considerations for healthcare providers in the United States. Clin Infect Dis. 2012;55:1:S10-5. (2). Shawcross DL, Shabbir SS, Taylor NJ et al., Ammonia and the neutrophil in the pathogenesis of hepatic encephalopathy in cirrhosis. Hepatology. 2010;51:1062-9. (3). Thames AD, Castellon SA, Singer EJ et al. Neurol Neuroimmunol Neuroinflamm. 2015:14;1. (4). Christopher L1, Koshimori Y1, Lang AE et al., Uncovering the role of the insula in non-motor symptoms of Parkinson's disease. Brain. 2014;137:2143-54. (5). Chang LJ et al., Decoding the role of the insula in human cognition: functional parcellationand large-scale reverse inference. Cereb Cortex. 2013;23(3):739-49.Figures
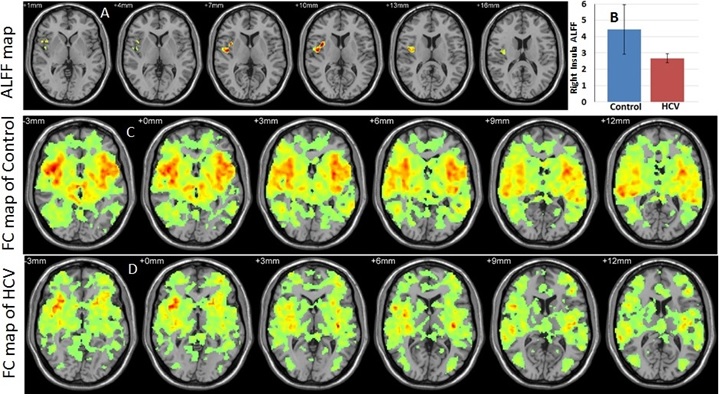
Fig.
1: Regions of ALFF differences between control and HCV (two sample t-test) (A).
Decreased ALFF in right insula of HCV patients (B). FC related to an ROI (right
insula) in control (C) and HCV (D) - (one sample t-test).