1686
Radiation-induced Brain Abnormalities: Plasticity, Progression and Outcome Prediction1Department of Radiology and BRIC, University of North Carolina at Chapel Hill, Chapel Hill, NC, United States, 2Department of Brain and Cognitive Engineering, Korea University, Seoul, Korea, Republic of
Synopsis
Brain plasticity is fascinating and important to our life. Radiation therapy can cause brain injury which may cover or progress, posing an ideal case to study brain plasticity. We used a rare and unique cohort of nasopharyngeal carcinoma patients with normal-appearing brains to study irradiation injury in its preclinical stage in context of brain functional and structural plasticity. We found an acute increase in local brain activity, followed by its extensive reduction; and significant functional connectivity loss in the default mode network. Such radiosensitive functional alterations were intriguingly found to be plastic. By contrast, a progressive late disrupted integrity of the related white matter was starting to be significant after one year at the far end. Early increased local brain functional activity was able to predict severe later brain necrosis through a bridge of brain connectome. These findings highlight the importance of brain connectomics in translational clinical study.
Introduction
RT is a longstanding and routine clinical treatment for cancer. During cranial RT, normal brain tissue along the RT pathway and in proximity to tumours is inevitably irradiated, causing not only transient and reversible abnormalities but also progressive and irreversible late toxicities such as brain tissue necrosis. Preclinical detection of the irradiation injury, when no MR-visible lesions are developed, is of great importance in the early prevention or mitigation of these complications. The major constraints of such studies have been: 1) a short survival time for brain tumour patients that leaves us a limited follow-up time to investigate late responses, and 2) residual brain lesions or recurrences that may not be easily differentiated from RT-induced injuries. Nasopharyngeal carcinoma patients constitute an ideal cohort for such a study and can avoid the aforementioned problems. This study is to explore RT-induced brain injuries in the preclinical stage in a voxel-wise manner and to characterize their evolutional process.Materials and Methods
87 patients were involved (44.22 9.85 years; range: 19-68 years; 23 females). For details, please see Table 1. Sixty-two patients had been treated with RT. Based on the time between RT completion and MRI acquisition, subjects were divided into four groups (G1, G2, G3, and G4; N = 25, 24, 19 and 19, respectively). We collected two non-invasive imaging modalities, rs-fMRI and DTI for each patients. We first conducted comparisons on local brain activity using fALFF maps. We then compared whole brain long-range co-activity using FC analysis with the seed defined at the PCC. Next, white matter microstructural integrity were compared using FA Analysis. The comparisons were carried out between post-RT groups (G2, G3, and G4) and the pre-RT group (G1) using separate two-sample t-tests. Regarding the relationship between post-RT brain functional and structural changes, we tested the hypothesis that changes in local brain activity could occur with or be followed by a disrupted FC and/or reduction of white matter microstructural integrity using DTI tractography. For patients in G2, G3 and G4, we conducted follow-up observations with clinical MRI. Based on whether or not temporal lobe necrosis happened in next five years after RT completion, we can retrospectively inspect the earlier brain functional/structural changes in the preclinical stage to search for any predictive biomarker or early sign of severe RT-injury.Result
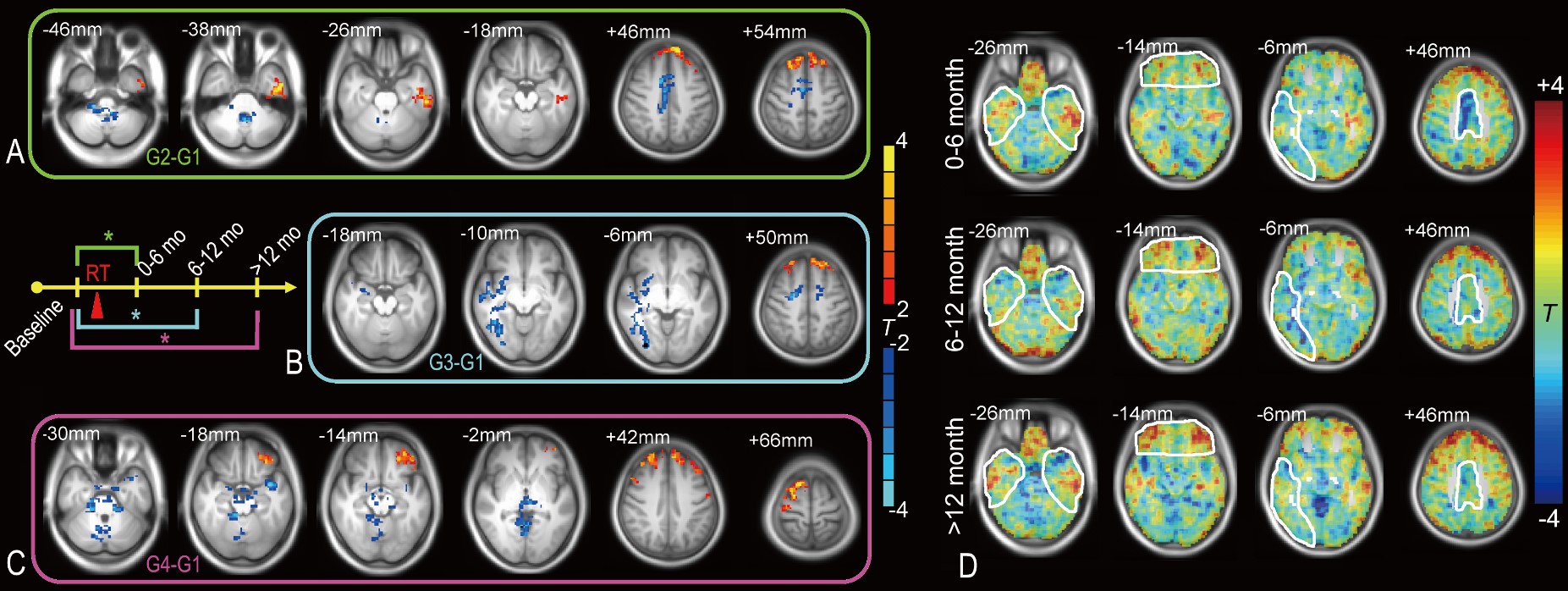
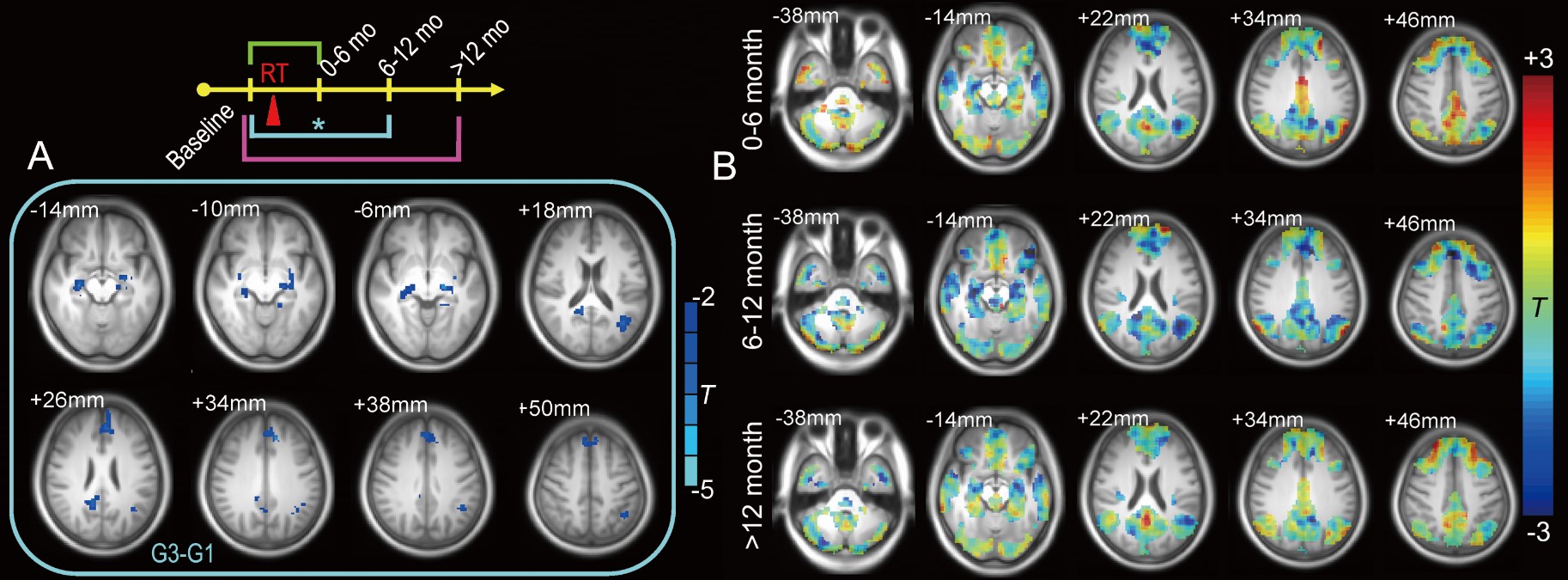
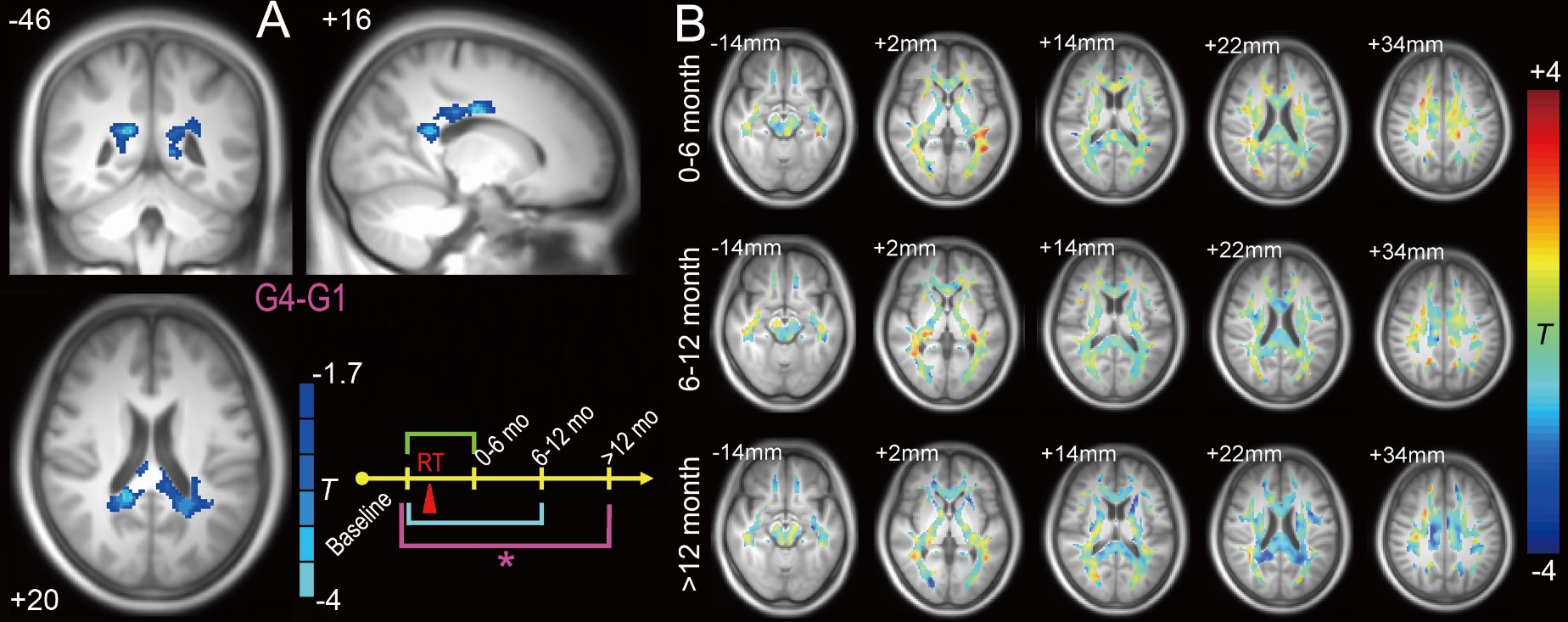
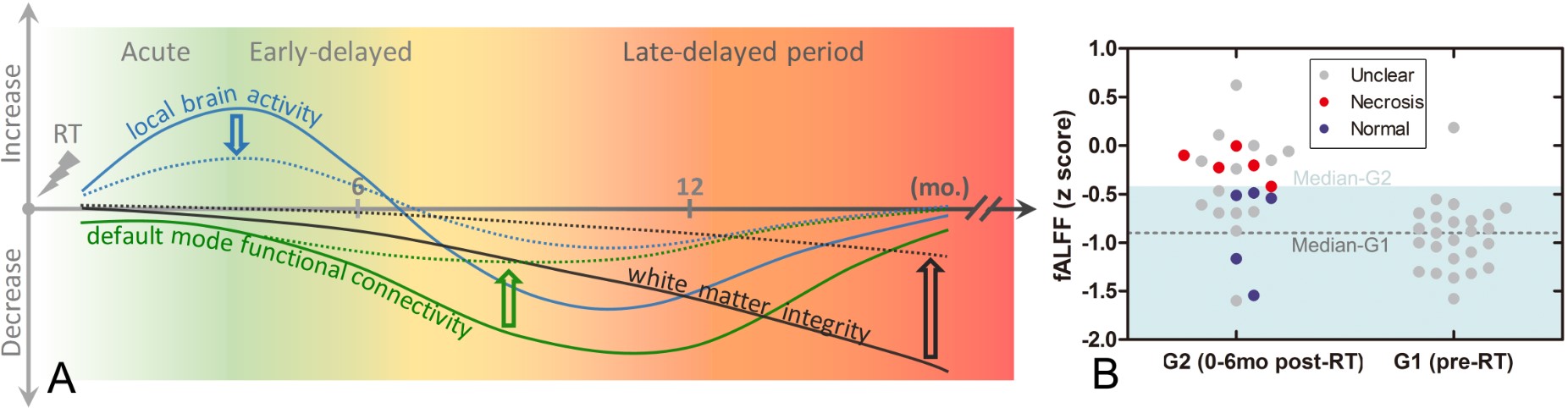
Compared with the baseline pre-RT group (G1), subjects in G2 (0 to 6 months after RT) had increased fALFF in the left inferior temporal areas. G2-G1 also showed a fALFF increase in the superior frontal area and a fALFF decrease in the supplementary motor area. G3-G1 showed a significant extensive decrease in the fALFF in the dispersed right temporal area and part of the supplementary motor area (Fig. 1). There were no significant differences for G2-G1 and G4-G1. However, G3-G1 revealed a reduced FC with the PCC at various DMN regions (Fig. 2). Within an FA mask in putative white matter, there was a significant reduction in the FA value in G4-G1 (Fig. 4A) but not in G3-G1 or G2-G1 (Fig. 3). Based on the above statistical analysis results, the schematic recovery/progression course could be plotted and we derived a hypothesis to prevent or delay late effects, which is called “preventive model” (Fig. 4). We also found fibers that connect between earlier functional and later structural changes. There was a significant correlation between the PCC-to-right hippocampus FC and the maximum dose applied to the right temporal lobe (r = 0.66, p < 0.05). The higher the maximum dose, the lower the FC strength would be.Conclusion
By using a precious multimodal brain imaging data, we revealed how the post-radiotherapy brain undergoes, in preclinical stage, an evolutional process with both functional and structural changes as well as both plastic recovery and progression. We have proposed a dynamic process in the post-RT brain with earlier vasculopathology dominance and later demyelination dominance. Our results suggest both progressive white matter degeneration from near- to far-end and neuroprotective processes and compensatory effects involve in this recovery/progression course. Our preventive model highlights the importance of preclinical brain function monitoring, careful RT-dose tailoring and timely preventive neuroprotection for avoiding irreversible severe complications that worsen outcomes.Acknowledgements
No acknowledgement found.References
No reference found.Figures