1604
The presence of newly defined classical features of intraneural perineurioma may obviate the need for fascicular biopsy and pathologic diagnosis1Neurosurgery, Mayo Clinic, Rochester, MN, United States, 2Radiology, Mayo Clinic, Rochester, MN, United States, 3Radiology, Mayo Clinic, 4Neurosurgery, Mayo Clinic, Rochester, MN, 5Radiology, Mayo Clinic, Rochester, MN
Synopsis
Intraneural perineurioma is typically diagnosed by targeted fascicular biopsy and histopathologic analysis. Through review of clinical history and magnetic resonance imaging of consecutive patients undergoing fascicular biopsy, we define the classical features of intraneural perineurioma as no cancer history, unifocal disease, moderate-severe T2 hyperintensity, moderate-severe contrast enhancement, homogeneous contrast enhancement, fusiform shape, and enlargement of involved nerves. This combination of features has a high specificity and moderate sensitivity for the diagnosis of perineurioma. When the classical features of perineurioma defined in this study are present, the high specificity of this combination of features may obviate the need for fascicular biopsy.
PURPOSE
Intraneural perineurioma is a benign neoplasm derived from the perineurium of peripheral nerves. Diagnosis is typically made via targeted fascicular biopsy of the affected nerve and histopathologic analysis. The aim of the current study was to determine if the magnetic resonance imaging (MRI) combined with the clinical features of intraneural perineuriomas are diagnostic based on a large cohort, and second, to determine if clinical assessment and MRI alone are sufficient for diagnosis obviating the need for targeted fascicular biopsy.METHODS
Consecutive patients undergoing targeted fascicular biopsy between 2004 and 2010 were retrospectively identified. Patients with a non-diagnostic biopsy were excluded. The MRI immediately prior to the fascicular biopsy was reviewed for each patient. Data collected included age, sex, clinical presentation, history of cancer, pathologic diagnosis, signal intensity on T1-weighted, T2-weighted, and presence and pattern of enhancement on post-gadolinium fat saturated images, shape of the lesion, uni- versus multi-focality, whether involved nerves were enlarged, evidence of fatty muscular atrophy or subacute denervation changes in the associated nerve territory. Pathologic diagnosis was dichotomized to intraneural perineurioma and other. The outcome of interest was the set of features predictive of a diagnosis of intraneural perineurioma. Univariate logistic regression analysis was performed to test each variable for its ability to predict a diagnosis of perineurioma. The rpart statistical package in R was then used to create a classification tree for the diagnosis.RESULTS
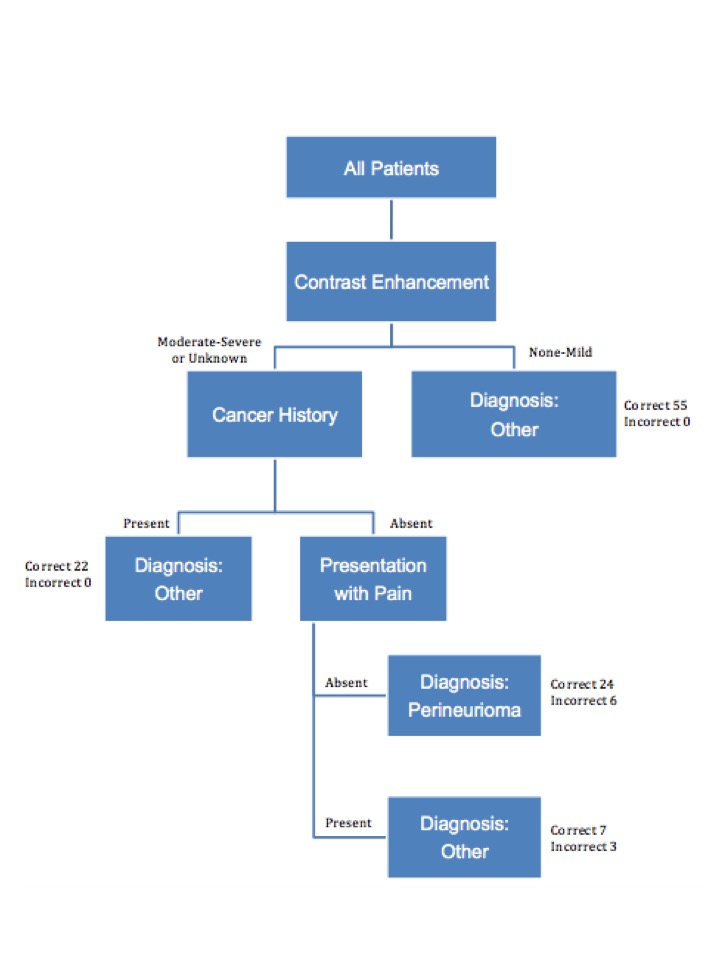
A total of 117 patients were included in the study; 27 had a pathologic diagnosis of intraneural perineurioma. Factors predictive of a diagnosis of perineurioma included moderate-severe contrast enhancement (OR 38.70, 95% CI 7.42 – 713.47, p<0.001), homogeneous contrast enhancement (OR 19.06, 95% CI 4.79 – 128.85, p<0.001), and fusiform shape (OR 4.55, 95% CI 1.22 – 29.58, p=0.02). Factors reducing the likelihood of a diagnosis of perineurioma included history of cancer (OR 0.05, 95% CI 0.003 – 0.23, p=0.003), presentation with pain (OR 0.23, 95% CI 0.05 – 0.71, p=0.009), and multi-focality (OR 0.09, 95% CI 0.005 – 0.43, p=0.001). We defined the classical features of intraneural perineurioma to be no cancer history (27/27 perineurioma group), unifocal disease (27/27), moderate-severe T2 hyperintensity (22/27), moderate-severe contrast enhancement (20/20 in patients in whom contrast was given), homogeneous contrast enhancement (18/20 in patients in whom contrast was given), fusiform shape (25/27), and enlargement of involved nerves (27/27). Classical features were present in 24 patients; 21 diagnosed with perineurioma and 3 with another diagnosis. The sensitivity of the classical features was 78% and specificity 97%. For the 3 false positives, the actual diagnoses were traumatic neuroma, microvasculitis, and glomangiomyoma. We utilized R to construct a classification tree based on the rpart algorithm (Figure 1). Features included in the classification tree were severity of contrast enhancement, history of cancer, and clinical presentation with pain. Sensitivity of the classification tree was 89% and specificity 93%.DISCUSSION
Classical features of intraneural perineurioma defined in this study included no cancer history, unifocal disease, moderate-severe T2 hyperintensity, moderate-severe contrast enhancement, homogeneous post-gadolinium contrast enhancement, fusiform shape, and enlargement of involved nerves. This combination of features had a high specificity with moderate sensitivity, and thus is conservative as a diagnostic algorithm with few false positives. The classification tree created here had an improved sensitivity but poorer specificity in comparison to the classical features. In order to obviate the need for biopsy and avoid misdiagnosis, the specificity needs to be high. The sensitivity in this case is less important since false negatives would be captured with biopsy. As a result, the classical features outperformed the classification tree, since the specificity was higher.CONCLUSION
When the classical features of perineurioma defined in this study are present, the high specificity of this combination of features may obviate the need for fascicular biopsy and pathologic diagnosis. Fascicular biopsy should continue to be performed when any of the classical features are absent.Acknowledgements
No acknowledgement found.References
No reference found.Figures