1595
Three-dimensional fracture visualization with Zero Echo Time MRI1GE Healthcare, Cambridge, United Kingdom, 2University Hospital of Zurich, Zurich, Switzerland
Synopsis
The present study is aimed at assessing the performance of proton density-weighted zero-echo time (ZTE) acquisition for the visualization of bone fractures.
Purpose
Sequences and post-processing methods capable of time-efficient MR-based bone delineation have evolved considerably in the past few years1-3. A new bone imaging technique, based on proton density-weighted, single-echo zero-echo time (ZTE) acquisition has recently been developed for PET/MR attenuation correction4. The present study is aimed at assessing the performance of said technique for the detection of bone fractures.Methods
A prototype zero echo time 3D radial sequence enabling high-bandwidth acquisition was deployed at a SIGNA PET/MR scanner (GE Healthcare, Waukesha, WI). The acquisition protocol, similar to that described by Wiesinger et al4, was set up: pixel size=(1-2mm)2, slice thickness=1-2mm, FA=1deg, BW=±62.5kHz, NEX=4, with field-of-view and receive coil individually adapted for each anatomical region. The post-processing consisted of automated bias correction, background suppression and intensity rescaling, resulting in CT-like images proportional to tissue density.
The patient cohort consisted of: Seven cases of surgical alterations of the skull, for which CT data were available; One case of multiple traumatic metatarsal fractures, acquired at three different time points during the healing process under conservative treatment and for which CT data were available; One case of multiple traumatic fractures of the pelvis, imaging acquired after surgical reconstruction.
Side-by-side ZTE and CT data were inspected by a radiologist with 8 years of experience. Corresponding fracture lines and other bone alterations (e.g. detached fragments) were identified.
Results
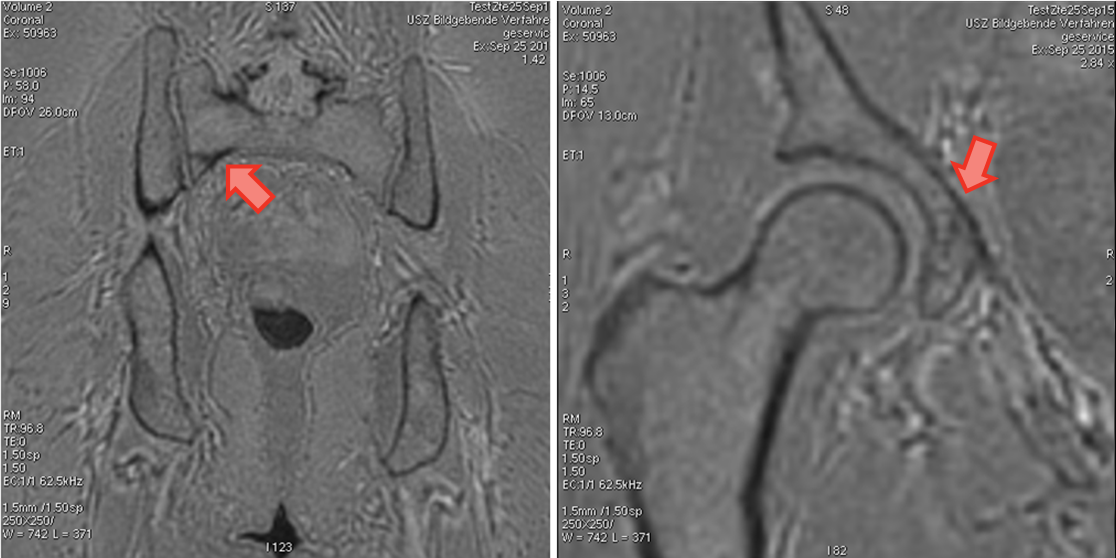
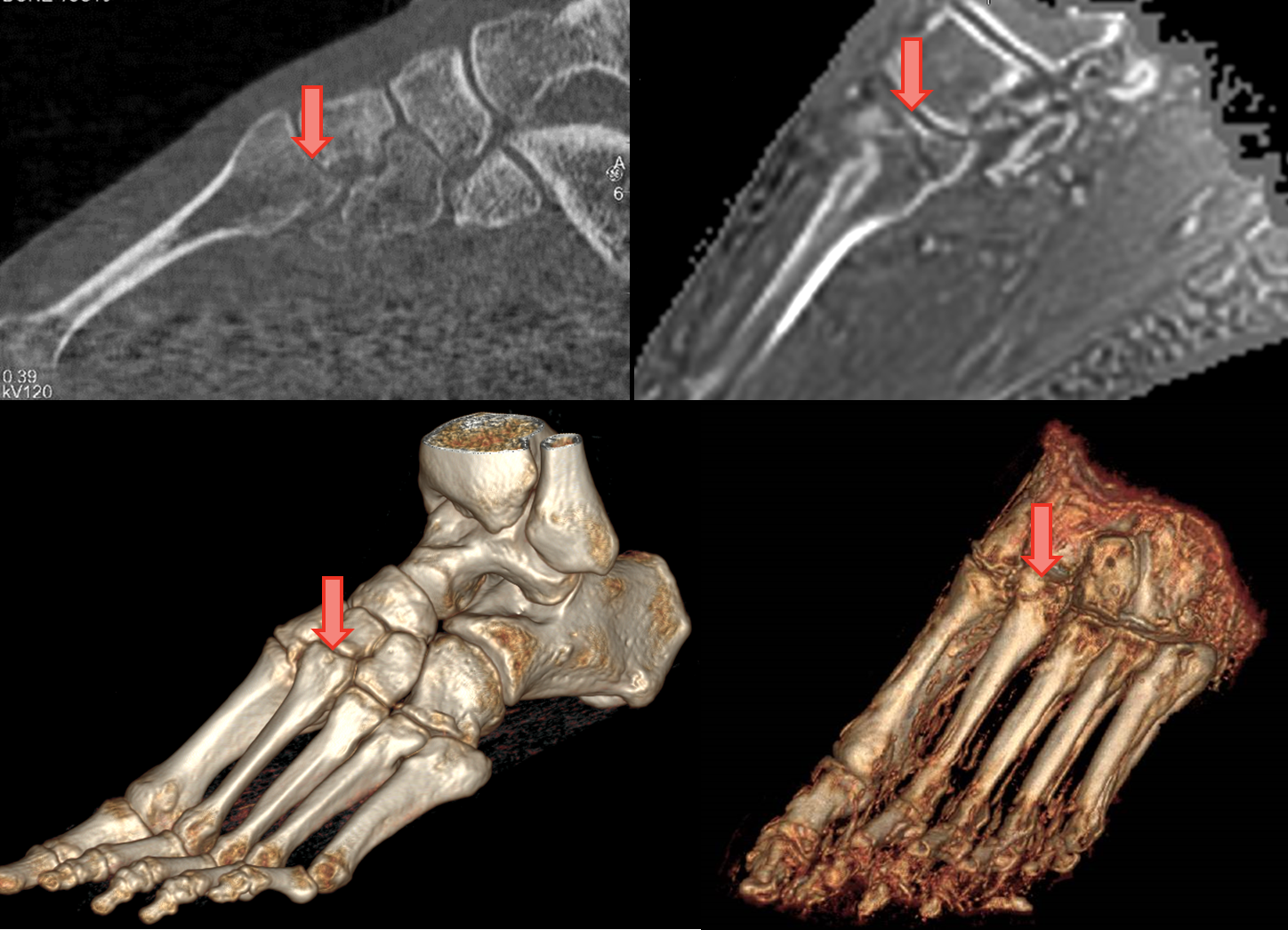
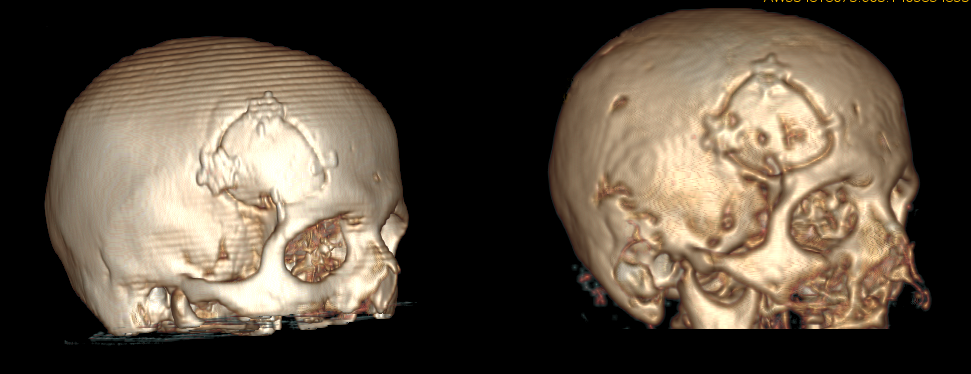
Figures 1-3 illustrate the obtained results on traumatic pelvic and metatarsal fractures, and on surgical alterations, respectively. In all cases the fracture lines / osteotomy margins were clearly visible on both CT and ZTE data, even in the absence of displacement. In the particular case of the metatarsal fractures, the lesions were more salient in the MR datasets than in the clinically indicated CT. Isolated bone fragments were also seen in the vicinity of the lesion. For all other cases the results were equivalent. Conventional MR sequences were judged superior in the depiction of recent lesions, due to the accumulation of fluid on the fracture interface, but their non-functional relation with tissue density made them impractical for three-dimensional visualization.
The identification of bone with thin cortical layer remains challenging, due to the tradeoff between voxel size and acquisition averaging required to compensate the reduced SNR. Cortical thicknesses below 1mm remained visible in the standard views but became hard to capture in rendered views due to partial volume effects.
Discussion
Limited previous work has been reported on the use of ultra-short echo time (UTE) sequences for bone fracture assessment5,6. To the best of our knowledge, this is the first study of ZTE-based fracture imaging. This technique offers the possibility to perform repeated follow-up acquisitions of complex fractures with a radiation-free method. Furthermore, being able to differentiate bone marrow from cortex, it may offer the possibility to evaluate fracture risks in patients with cortical erosions (e.g. due to metastases).
A full comparison with recently published results6 was, for the time being, prevented by an intrinsic restriction of the pulse sequence, which prevents excessively long acquisition times (8-16 minutes were reported by Wu et al). A modified version of the sequence has been developed to enable this comparison. Ongoing work is underway to extend the present study to a larger sample, including both recent and healed fractures.
Conclusion
The preliminary results obtained in this study suggest that the detection of bone fracture with zero echo time MRI is possible, providing a potential alternative to CT imaging, particularly in cases where soft-tissue information is relevant or requiring repeated multiple follow-up scans.Acknowledgements
No acknowledgement found.References
1. Du et al, Magn Res Ima. 2011; 29:470–482
2. Keereman et al, J Nucl Med. 2010; 51:812-818.
3. Grodzki et al, Magn Res Med.2012; 67:510-518
4. Wiesinger et al, Magn Res Med. 2016; 75(1):107-14.
5. Reichert et al, Magn Res Ima. 2005; 23:611-618.
6. Wu et al, Eur Radiol. 2016; 26(1):138-46.
Figures