1582
Diffusion Tensor imaging in the Injuries of the Levator Ani Muscle in Female Pelvic Floor Dysfunction1Radiology Department of Peking University Third Hospital, Beijing, People's Republic of China, 2GE Healthcare, MR Research China, BeiJing, People's Republic of China
Synopsis
To find the most vulnerable component of levator muscle, this research compared the levator ani muscle which contains pubovisceral, puborectal and iliococcygeal muscles between the control group and the patient group by using DTI. 49 female PFD (pelvic floor dysfunction) patients and 51 female healthy subjects underwent DTI imaging on a 3.0T MR system. A significant difference was found in the FA value of the right pubovisceral muscle between the two groups, and therefore, this part are more likely to be damaged comparing with other compartments of levator ani muscle. DTI with fiber tractography permits the evaluation of the injuries of levator ani muscle, which has a certain effect in revealing the pathogenesis of the female pelvic floor dysfunction.
Purpose
Diffusion tensor imaging (DTI) with fiber tracing technique has been applied to display the anatomy and functions of skeletal muscles [1, 2]. To determine the feasibility of using DTI with fibre tractography as a tool for evaluating the injuries of levator muscle, this research will compare the levator ani muscle which contains pubovisceral muscle, puborectal muscle and iliococcygeal muscle between the control group and the patient group by using DTI. The purpose of this work was to find the most vulnerable component of levator muscle and to make the fiber tractography of levator ani muscle.Material and Methods
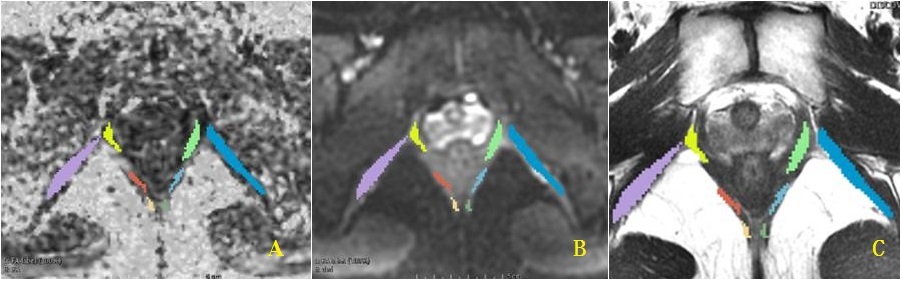
Forty-nine female PFD patients (mean age 61±12 years, eutocia, mean BMI 25.06, PFD diagnosed by a urogynecologist with 30 years’ experience) and fifty one female healthy subjects (mean age 62±6.4 years, eutocia, mean BMI 24.89) underwent DTI on a 3.0T MR system(GE Discovery MR 750). Conventional MRI sequences were performed in all subjects, including sagittal, axial, coronal FRFSE T2WI and axial FRFSE T1WI. The DTI acquisition, with an overall scan of 4 min 19s, used a two-dimensional diffusion weighted spin echo imaging (SE-EPI): axial plane, 20 slices with 5mm thickness and no gap, FOV = 40cm×32cm, matrix = 160×192, TR/TE = 4770/54 ms, b value = 500 s/mm2, 2 averages. Finally, the fast imaging employing steady-state acquisition(FIESTA) was performed to evaluate the severity of pelvic organ prolapse in the patient group, and to exclude the pelvic organ prolapse in the control group. The DTI data was analyzed using dedicated software named 3D slicer (www.slicer.org, Brigham and Women’s Hospital, Boston). After post-processing of the DTI data, fractional anisotropy (FA) map and mean diffusivity (MD) map were obtained (Figure.1A-C). The FA and MD values of both sides of pubovisceral muscle, puborectal muscle and iliococcygeal muscle were calculated independently. Permuscle means for MD and FA values were compared between the two groups using a Student t-test analysis. A p-value less than 0.05 was considered statistically significant. Fiber tracing for visualization of predefined pelvic floor and pelvic wall muscles was performed offline by two observers, applying a consensus method. Fractional anisotropy (FA) and mean diffusivity (MD) were calculated from the fiber trajectories.Results
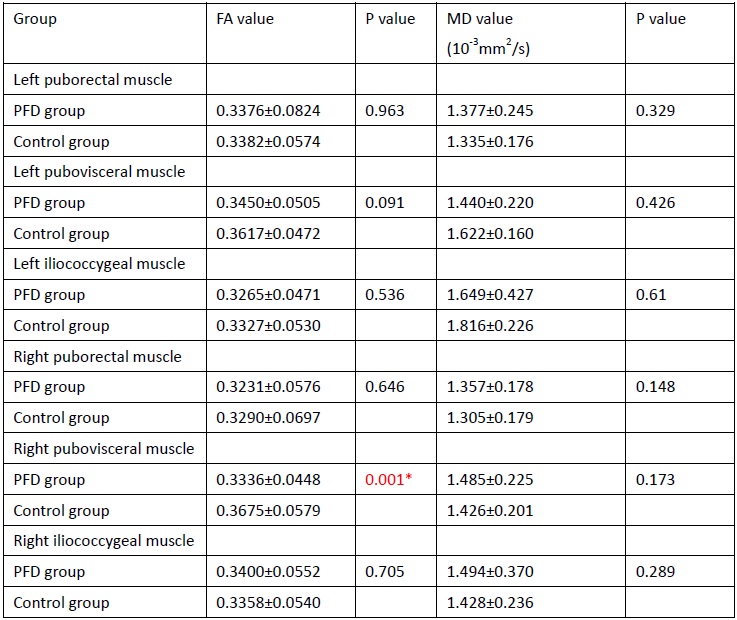
The results are shown in Table 2. A significant difference was found in the FA value of the right pubovisceral muscles between the two groups. There was no statistically significant difference (P>0.05) for the FA value of the left pubovisceral muscles, two sides of puborectal muscle or iliococcygeal muscle between the two groups. Furthermore, there was no statistically significant difference (P>0.05) for the MD value of both sides of pubovisceral muscle, puborectal muscle or iliococcygeal muscle between the two groups. Fiber-tracking resulted in a satisfactory representation of the global muscle morphology. The fibers of right pubovisceral muscles were decreased to a different degree, while the fibers of right pubovisceral muscles in the control group were morphologically intact and there was no significant atrophy or bundle fracture (Figure 2.a-b).Conclusion
Our research shows that a significant difference was found in the FA value of the right pubovisceral muscles(p<0.05), which indicates that the right pubovisceral muscles are more likely to be damaged compared to other compartments of levator ani muscle. DTI with fiber tractography permits identification of the components of levator ani muscle and the evaluation of the injuries of levator ani muscle, which has a certain effect in revealing the pathogenesis of the female pelvic floor dysfunction [3]. Regardless of change in the morphology of levator ani muscle, the DTI parameters of right pubovisceral muscle decrease in PFD patients in comparison with healthy women.Acknowledgements
No acknowledgement found.References
[1] Budzik JF, Balbi V, Verclytte S, Pansini V, Le TV, Cotten A. Diffusion tensor imaging in musculoskeletal disorders. Radiographics. 2014. 34(3): E56-72.[2] Taylor SA. Imaging pelvic floor dysfunction. Best Pract Res Clin Gastroenterol. 2009. 23(4): 487-503.
[3] Rousset P, Delmas V, Buy JN, Rahmouni A, Vadrot D, Deux JF. In vivo visualization of the levator ani muscle subdivisions using MR fiber tractography with diffusion tensor imaging. J Anat. 2012. 221(3): 221-8.
Figures