1478
Free-Breathing T2-Weighted Abdominal Examination Using Radial 3D Fast Spin-Echo Imaging1Center for Advanced Imaging Innovation and Research (CAI2R), Department of Radiology, New York University School of Medicine, New York, NY, United States, 2Bernard and Irene Schwartz Center for Biomedical Imaging, Department of Radiology, New York University School of Medicine, New York, NY, United States, 3Department of Radiology and Medical Imaging, University of Virginia, Charlottesville, VA, United States, 4Department of Radiotherapy, University Medical Center Utrecht, Utrecht, Netherlands, 5Center of Advanced Imaging Innovation and Research (CAI2R), Department of Radiology, New York University School of Medicine, New York, NY, United States
Synopsis
A 3D fast spin-echo (FSE) sequence design for free-breathing T2-weighted abdominal examination is described. Due to use of radial stack-of-stars sampling, the sequence provides pure T2 contrast and achieves high robustness to motion, enabling that patients can be scanned during shallow breathing. Using an integrated FID navigator, the sequence can additionally be combined with the self-navigated XD-GRASP reconstruction principle for patients who perform deep breathing. Furthermore, the navigator can be used for bulk-motion detection. Initial results in a free-breathing adult volunteer are shown.
Introduction
MRI examinations of the abdomen are challenging because patients are traditionally required to suspend respiration during data acquisition, which leads to high failure rates. Therefore, free-breathing techniques have been developed that monitor the respiration with external sensors or navigators and try to acquire data with consistent respiratory state (“gating”)1. However, gated acquisitions are time-inefficient and fail frequently in clinical practice, either because of sensor inaccuracies or dynamic changes of the patient’s breathing pattern.
Lately, a new class of free-breathing techniques has been described that use radial sampling for data acquisition2. Because radial acquisition is inherently robust to motion and prevents appearance of typical MRI ghosting artifacts, diagnostic images can be obtained during shallow breathing without additional correction mechanisms. Most work so far, however, has been done for either static or dynamic T1-weighted imaging.
The purpose of this work is to describe our progress in developing a corresponding radial 3D Fast Spin-Echo (FSE) sequence for free-breathing T2-weighted abdominal examination.
Methods
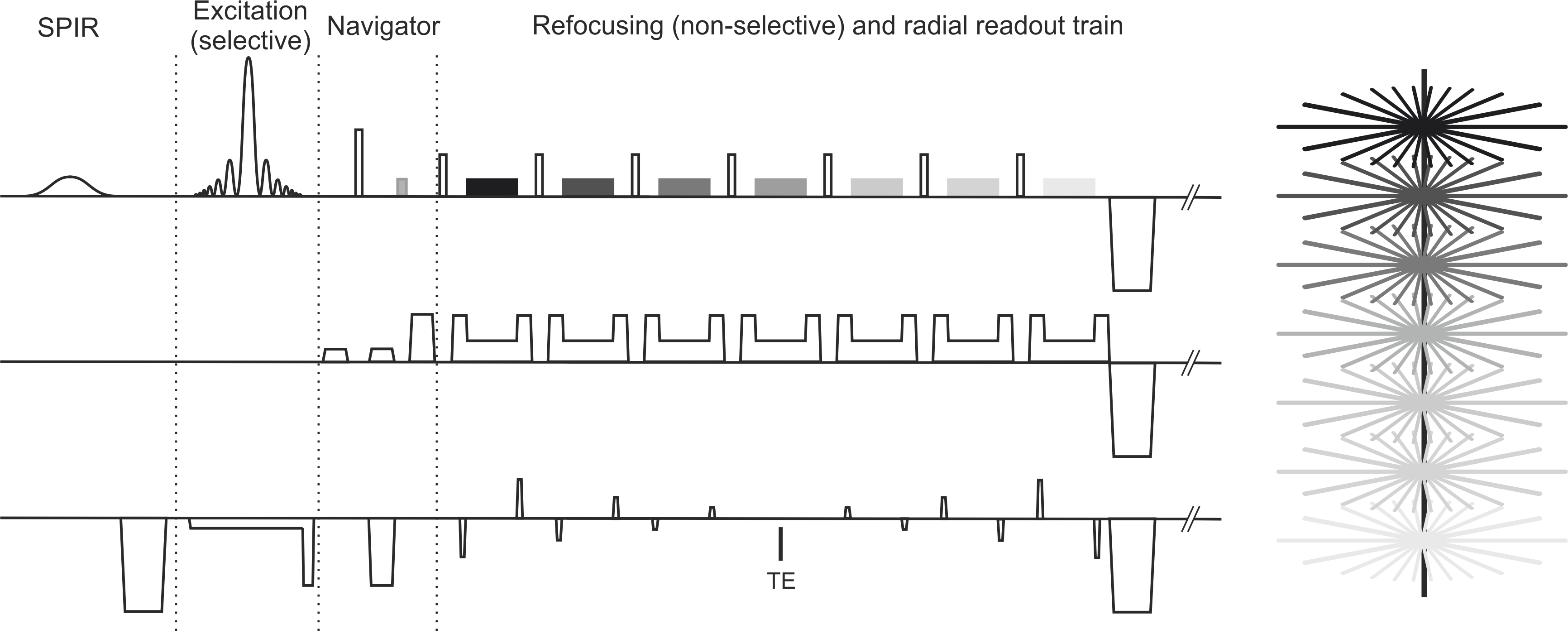
Due to the overlap of spokes in the k-space center, only a mixed PD/T2 contrast can be obtained with radial 2D FSE sequences. Therefore, a 3D FSE sequence design with stack-of-stars geometry was chosen (see Figure 1). By placing the echo train along the slice direction, pure T2 contrast is obtained, which is determined by the echo time of the center partition. Moreover, with a 3D acquisition, slice jumps are avoided for free-breathing scans, and the resulting imaging properties are similar to the related T1-weighted radial sequences.
Figure 1 shows the basic sequence diagram. Slab-selective excitation is used to avoid aliasing when scanning in axial orientation. Refocusing pulses are non-selective to shorten the echo spacing. The initial refocusing pulse uses a flip angle of 180o, while the remaining pulses use a smaller but fixed flip angle. Strong crusher gradients are placed around each refocusing pulse to eliminate spurious FID signals induced by pulse imperfections. Moreover, phase cycling between adjacent spokes is used to cause destructive interference of FID contributions in the overlapping projections. Bigger crushers are used around the initial refocusing pulse to spoil signals in vessels and improve sensitivity for lesions. Spectral Presaturation with Inversion Recovery (SPIR) is applied for fat suppression. The radial acquisition order follows the golden-angle scheme, which provides high flexibility for retrospective reconstruction. Furthermore, the initial spin echo is utilized to acquire a short FID navigation signal, which can be used for complementary respiratory-motion correction or bulk-motion detection.
Results
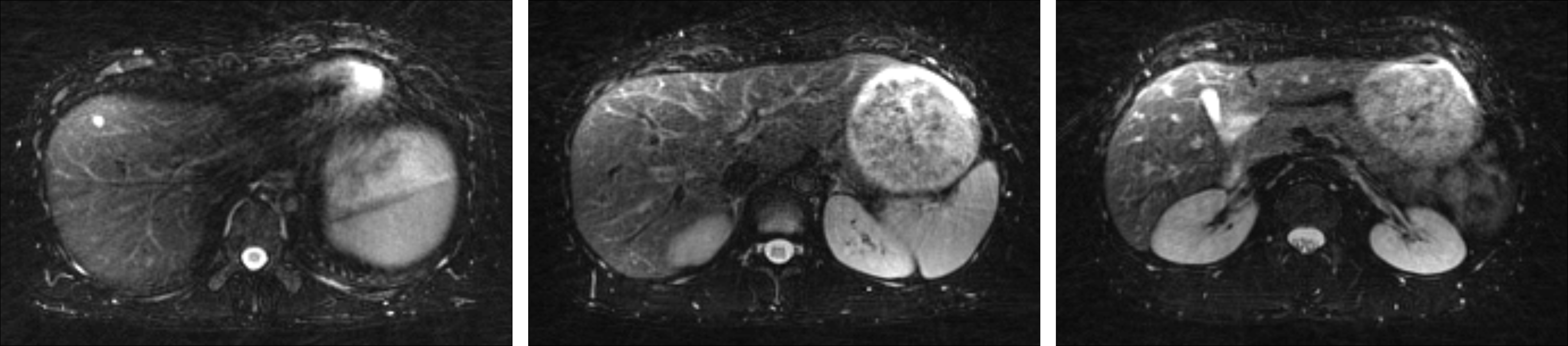
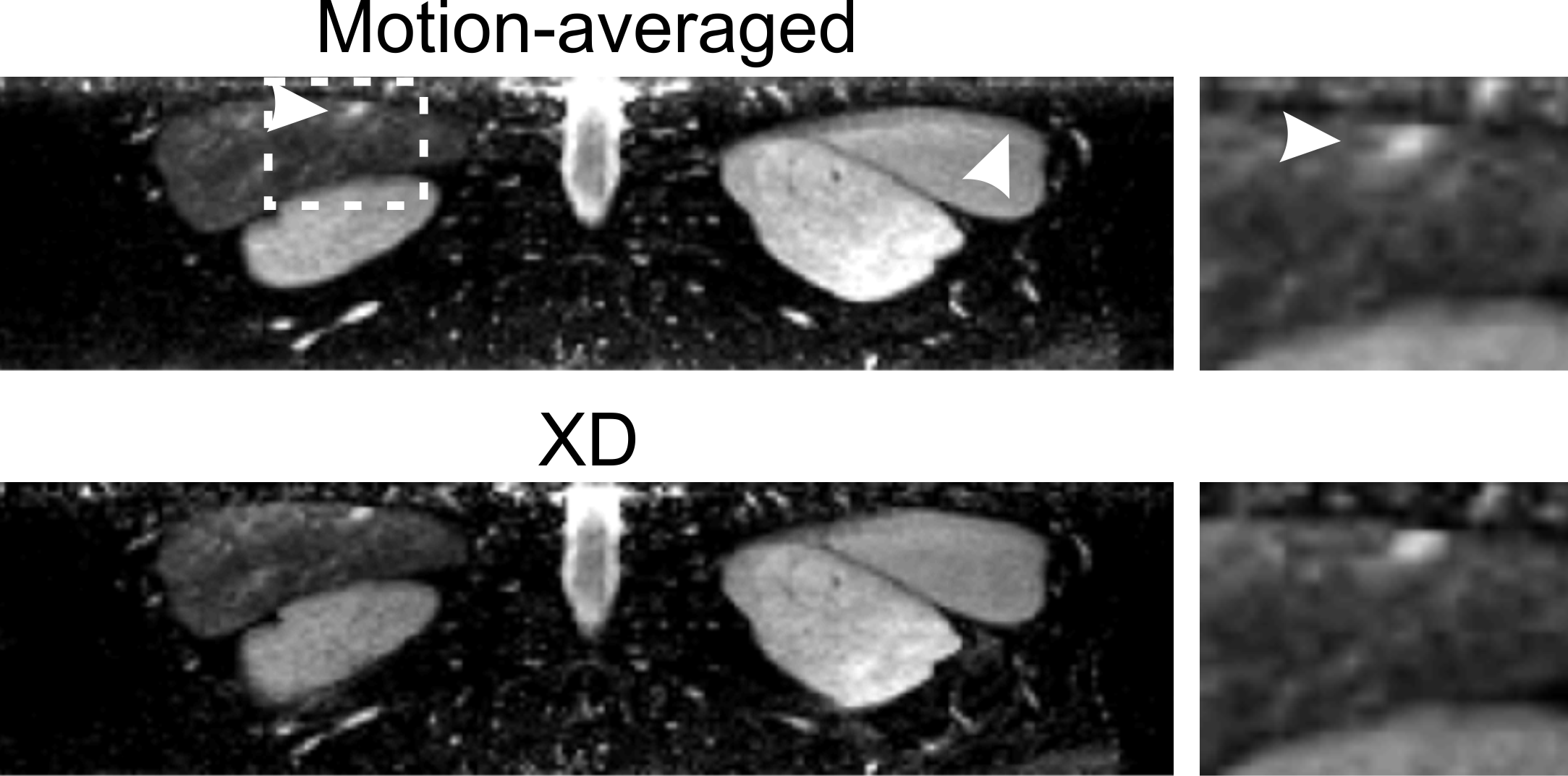
Figure 2 shows images from a fully-sampled free-breathing abdominal scan in an adult volunteer (MAGNETOM Aera 1.5T, 48 slices, 1.5x1.5x4mm3, BW 390Hz/px, FA 150o). 400 projections were acquired in 8min (TR/TE=1200ms/135ms). Figure 3 compares reconstructions with different undersampling factors, created by retrospective undersampling, as possible with the golden-angle scheme. Good image quality is remained, indicating that further scan acceleration is possible using parallel imaging or compressed sensing. Figure 4 shows results where the initial FID-navigation signal was utilized to correct for residual breathing motion using the XD-GRASP principle3. In XD-GRASP, respiratory motion is detected from the navigator and used to bin the data into different motion frames. Corresponding images are then reconstructed iteratively with total-variation regularization along the breathing dimension. It can be seen that the additional XD-GRASP respiration compensation leads to improved sharpness of a small cyst in the liver.Discussion and Conclusion
This work describes a new approach for free-breathing T2-weighted abdominal examination using radial stack-of-stars 3D FSE acquisition. The sequence provides pure T2 contrast and achieves reliable image quality without additional motion correction. Due to use of the golden-angle scheme and an integrated FID navigator, it is possible to further actively compensate for respiratory motion using the self-navigated XD-GRASP principle. This should provide diagnostic images also in patients who perform deep breathing. Furthermore, the integrated FID navigator can be used to detect bulk patient motion. Because of the radial undersampling behavior and the flexibility to reconstruct arbitrary windows from golden-angle sampling, it is then possible to adaptively reconstruct images only from motion-free phases of the acquisition.
One remaining limitation consists in the long acquisition time caused by the repetition delay, which is required for recovery of the longitudinal magnetization. Possible solutions include use of driven-equilibrium pulses, use of gradient- and spin-echo (GRASE)4 readout schemes where multiple spokes are acquired per echo, and use of compressed sensing. A second limitation consists in sporadic streaks that propagate from areas in the arms where fat suppression fails due to B0 inhomogeneities. In many cases, these artifacts can be removed by adaptively attenuating contributions from highly contaminated coil elements.
Acknowledgements
NIH P41EB017183, 5R01EB018308References
1. Klessen C et al., Magnetic resonance imaging of the upper abdomen using a free-breathing T2-weighted turbo spin echo sequence with navigator triggered prospective acquisition correction. J Magn Reson Imaging 2005;21:576-582
2. Block KT et al., Towards routine clinical use of radial stack-of-stars 3D gradient-echo sequences for reducing motion sensitivity. J Korean Soc Magn Reson Med 2014;18:87–106.
3. Feng L et al., XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing, Magn Reson Med, 75:775-788 (2016)
4. Gmitro AF et al., Radial GRASE: Implementation and Applications, Magn Reson Med, 53:1363-1371 (2005)
Figures