1403
Automated segmentation of Intramuscular Connective Tissue (IMCT) from skeletal muscle in presence of artifacts: Application to Changes in IMCT in an Unilateral Limb Suspension Induced Acute Atrophy Model in the Plantarflexors1Physics, San Diego State University, San Diego, CA, United States, 2Physics, UC San Diego, San Diego, CA, United States, 3Radiology, UC San Diego, San Diego, CA, United States
Synopsis
Chronic muscle atrophy can be induced by limb suspension and is characterized by a loss of muscle mass and force. However, there could also be changes to the connective tissue volume that may contribute to the loss of muscle function. We studied the changes in connective tissue volume in a model of chronic atrophy induced by Unilateral limb suspension (ULLS) using ultralow TE sequences. We integrated an artifact correction algorithm to a 3D fuzzy segmentation algorithm to automatically segment the connective tissue from dual echo UTEs images corrupted by artifacts. Percent connective tissue increased post-ULLS but not the absolute values.
Purpose
Structural changes in the muscle fiber are known to occur in chronic atrophy with these changes potentially linked to muscle function. Extracellular remodeling may also contribute to muscle force loss in suspension-induced atrophy. The intramuscular connective tissue (IMCT) can be visualized by the Ultralow TE sequences that can capture the short T2 signal of this collagenous tissue. We report an extension to an automated segmentation algorithm based on 3D fuzzy clustering with bias field corrections incorporating spatial connectedness to address a high frequency artifact (arising in regions of field inhomogeneities) that sometimes corrupt UTEs images. The study is focused on applying the extended segmentation algorithm to segment IMCT from the medial gastrocnemius to determine the changes in IMCT volume between baseline (pre-ULLS) and post-ULLS.Methods
Seven subjects were recruited for the acute atrophy study after IRB approval. Subjects were scanned prior to ULLS and just post-ULLS. The ULLS model included a 4 week unloading of the dominant leg using crutches and the non-dominant leg supported by a raised shoe. IMCT Quantification: Fat suppressed 3D Ultra Short Echo Time (3D Cones) sequence: four TEs 0.03ms/2.7ms/5.4ms/7.2ms, TR 71ms.1 The original algorithm is a 3D fuzzy clustering method that uses as input the multiple echo images of the UTEs acquisition, and structure tensor maps (that highlight the networked sheet like structure of the IMCT) created from the acquired multiple echo images.2 The extension to filter out the artifacts was implemented in the following steps: Structure tensor maps are generated from images that are blurred version of the acquired images and then thresholded to retain only the muscle voxels. These structure tensor maps are used to generate weight functions defined by:
$$$WF = 1- \exp(-\frac{ABS(ST_1-ST_2)}{\sigma(ST-AVE)})$$$
(where ST1 and ST2 are the structure tensor maps generated from the smoothed and thresholded images respectively and σ regulates real structure detection) to detect true features from artifacts. The artifact reduction is implemented within the bias field correction and is implemented iteratively and in each iteration, the smoothing mask size is changed in order to obtain an image free from artifacts (visually assessed). The artifact free images then serve as the input to the 3D fuzzy clustering algorithm.2
Results
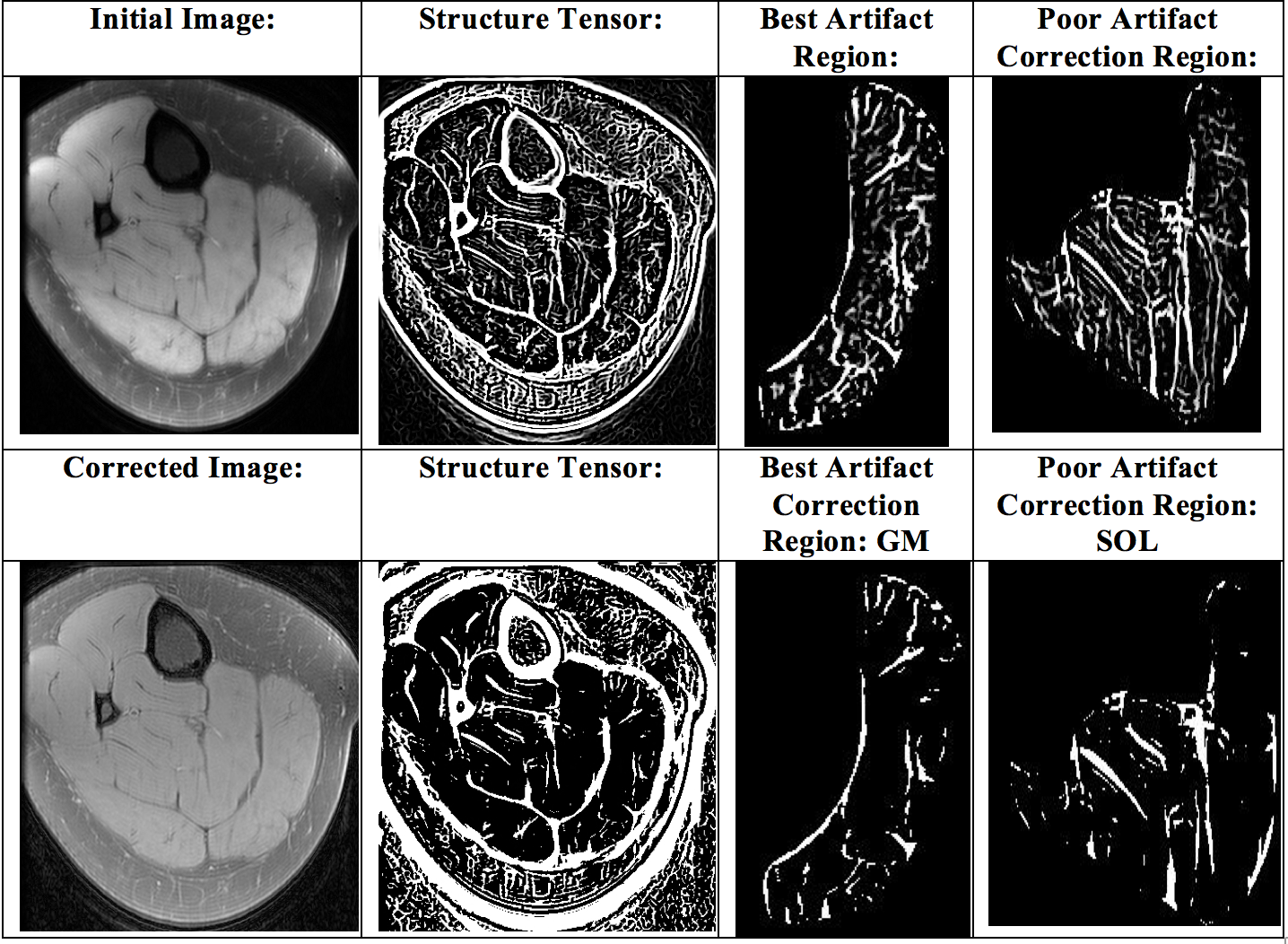
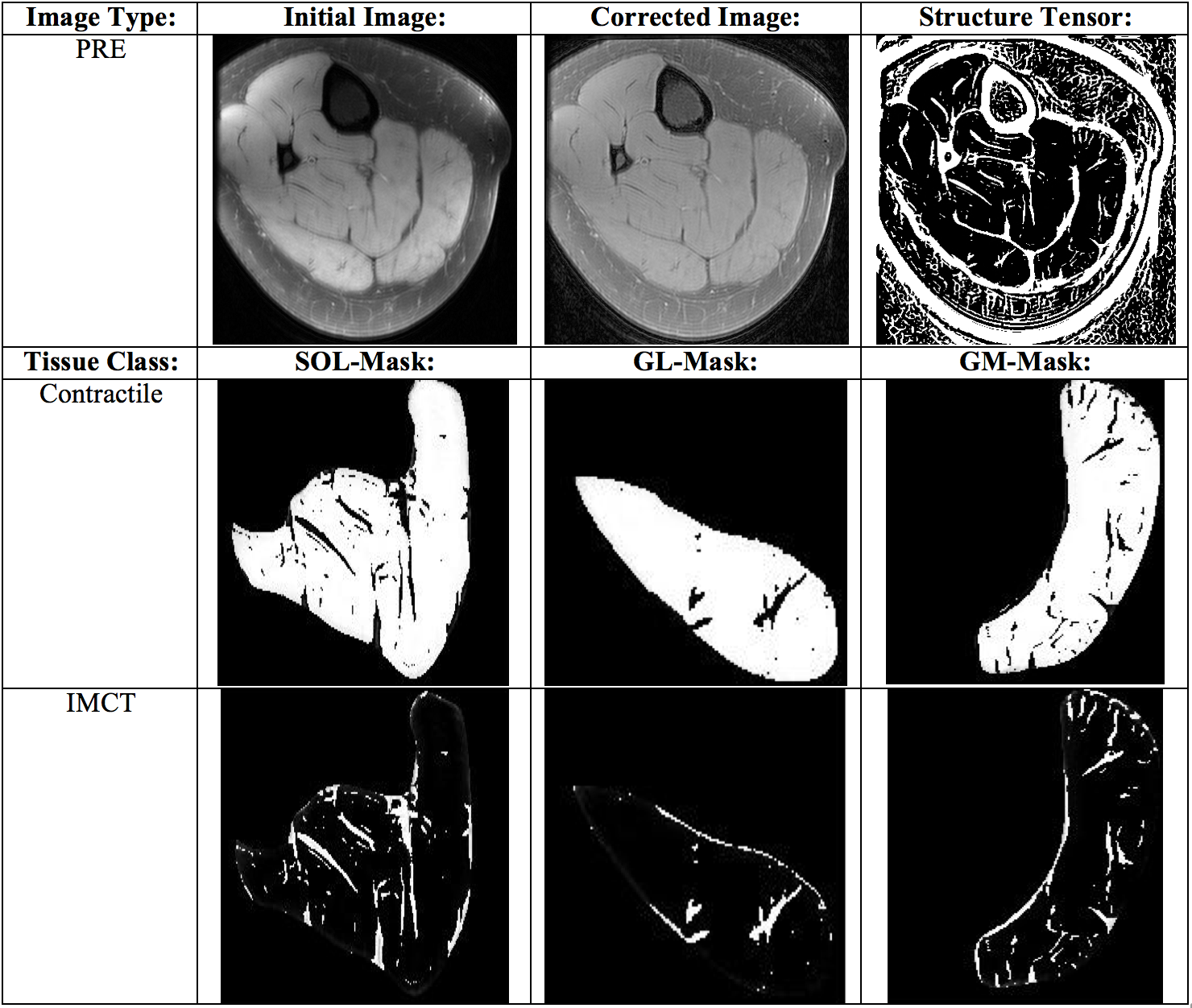
Figure 1 shows the images and the structure tensor (ST) images for the uncorrected and corrected data. The uncorrected ST images show the pronounced artifacts as high frequency ringing. These artifacts are not seen in the corrected ST images, confirming the efficiency of our algorithm in handling such structured artifacts. Fig. 2 shows the segmented images of the connective and contractile tissue for one subject in the pre- and post-ULLS condition. Table 1 is a preliminary result of the % contractile and % connective tissue after the application of the artifact correction extension to the 3D fuzzy clustering segmentation algorithm for two subjects (pre- and post ULLS).Discussion
Artifacts as seen in the UTEs images reported here can arise for a variety of reasons, especially in sequences that place a heavy demand on the scanner hardware. These images are acceptable for qualitative assessment as the artifacts can be distinguished readily from true features of the image by the human observer. However, it can be confounding for an automated segmentation algorithm. We have extended our segmentation algorithm to detect the artifacts and successfully applied to four image volumes. The proposed approach can be integrated with any other segmentation algorithm as well as for different types of artifacts (the value of sigma has to be adjusted for the specific artifact). The % connective tissue increases with limb suspension in all the three plantarflexor muscles primarily from the % decrease in contractile tissue (atrophy of the muscle fibers). That there was no change in the absolute amount of connective tissue was confirmed from the fact that normalized values (to pre and post muscle volumes) did not change between baseline and post-suspension.Conclusion
A robust artifact reduction technique was implemented to decrease the high frequency artifacts in UTEs images of the lower leg. It was integrated successfully into a fuzzy segmentation algorithm to determine the % changes in the connective tissue from UTEs images in post-limb suspension compared to baseline.Acknowledgements
This work was supported by National Institute of Arthritis and Musculo- skeletal and Skin Diseases Grant 5RO1-AR-053343-08.References
[1] Du J, Sinha, S, Chung, C, Bydder, G. Radiological Society of North America 2007 Scientific Assembly and Annual Meeting; Chicago IL2007.
[2] Ugarte V, Sinha U, Malis V, Csapo R, Sinha S. Magn Reson Med. 2016 Feb 19. doi: 10.1002/mrm.26156.
Figures