1344
Optimal MRI sequences for 68Ga-PSMA-11 PET/MRI in evaluation of biochemically recurrent prostate cancer1Radiology and Biomedical Imaging, UCSF, San Francisco, CA, United States, 2Urology, UCSF, San Francisco, CA, United States, 3Medicine, Division of Hematology and Oncology, UCSF, San Francisco, CA, United States
Synopsis
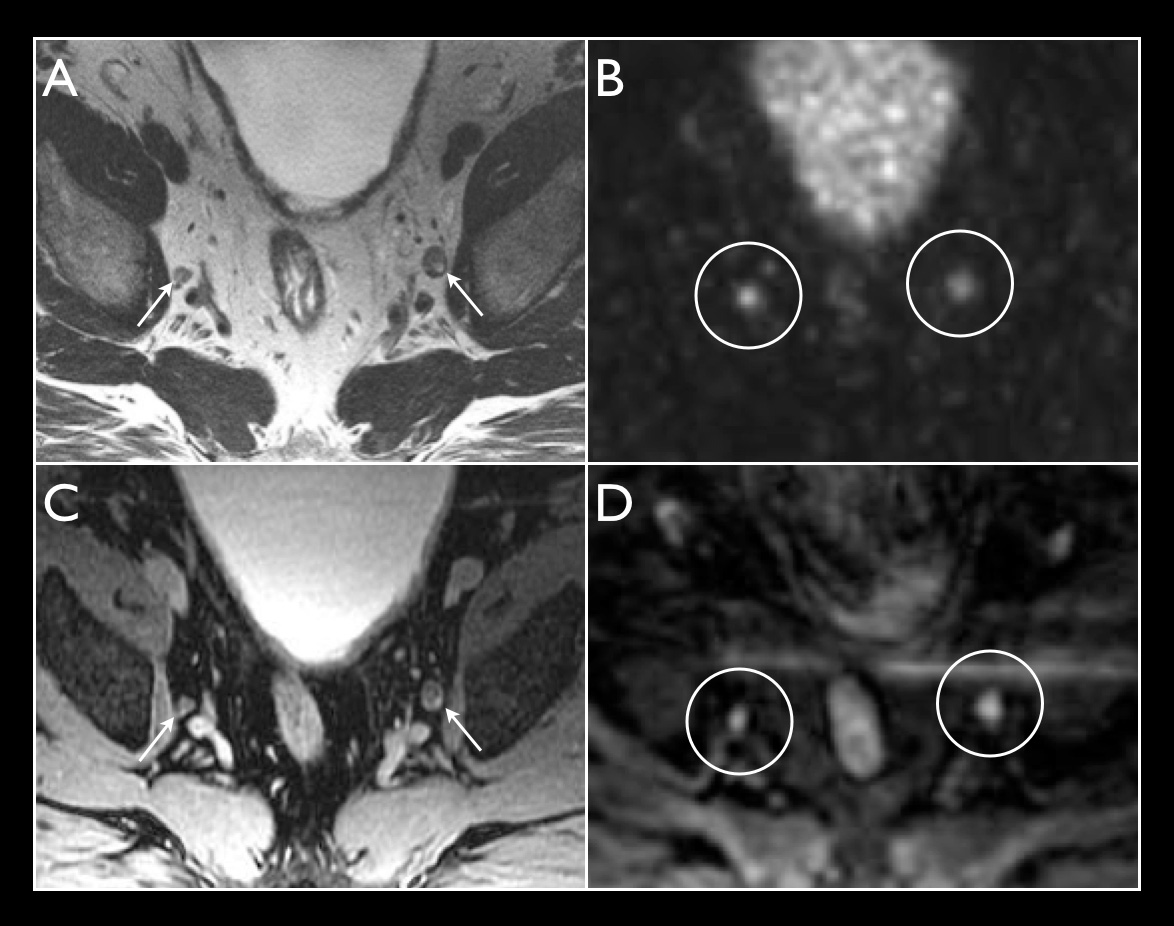
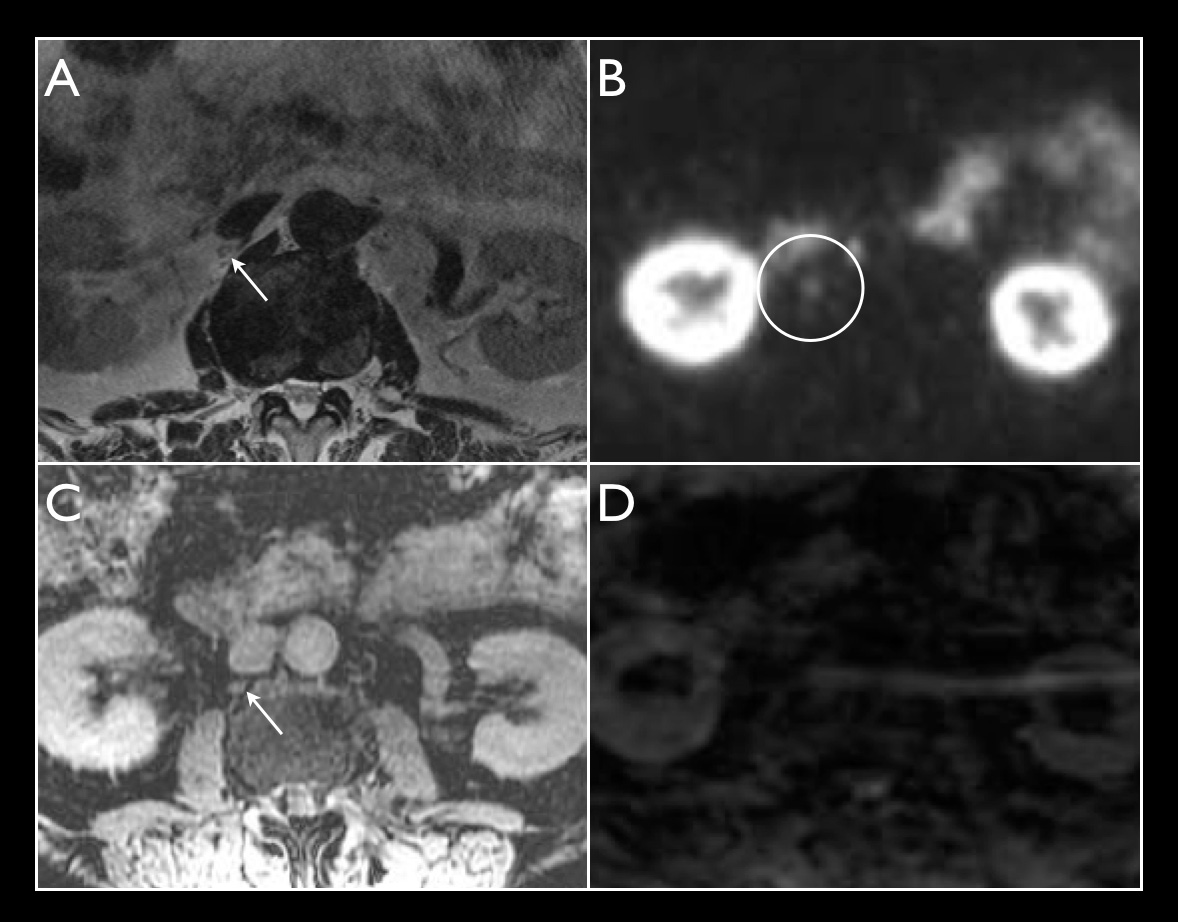
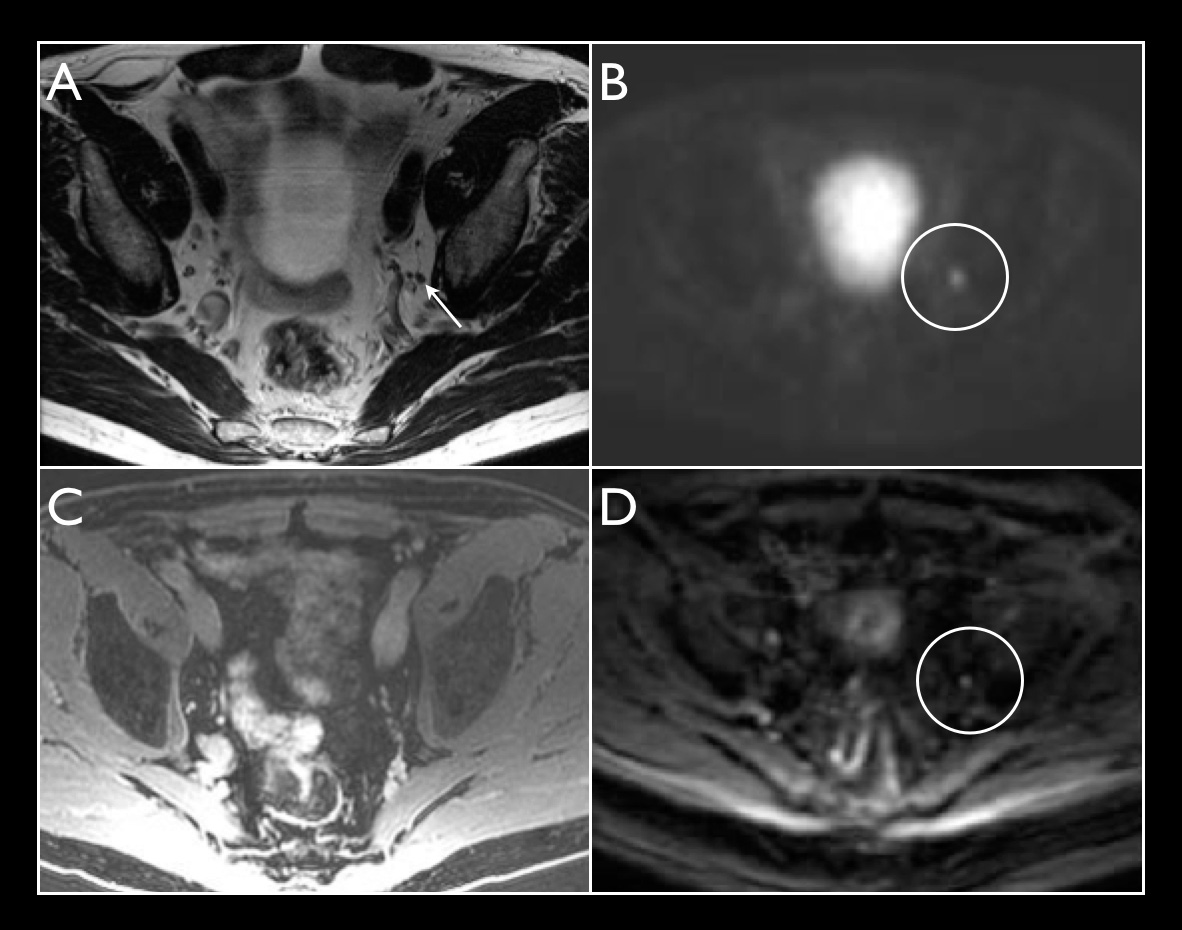
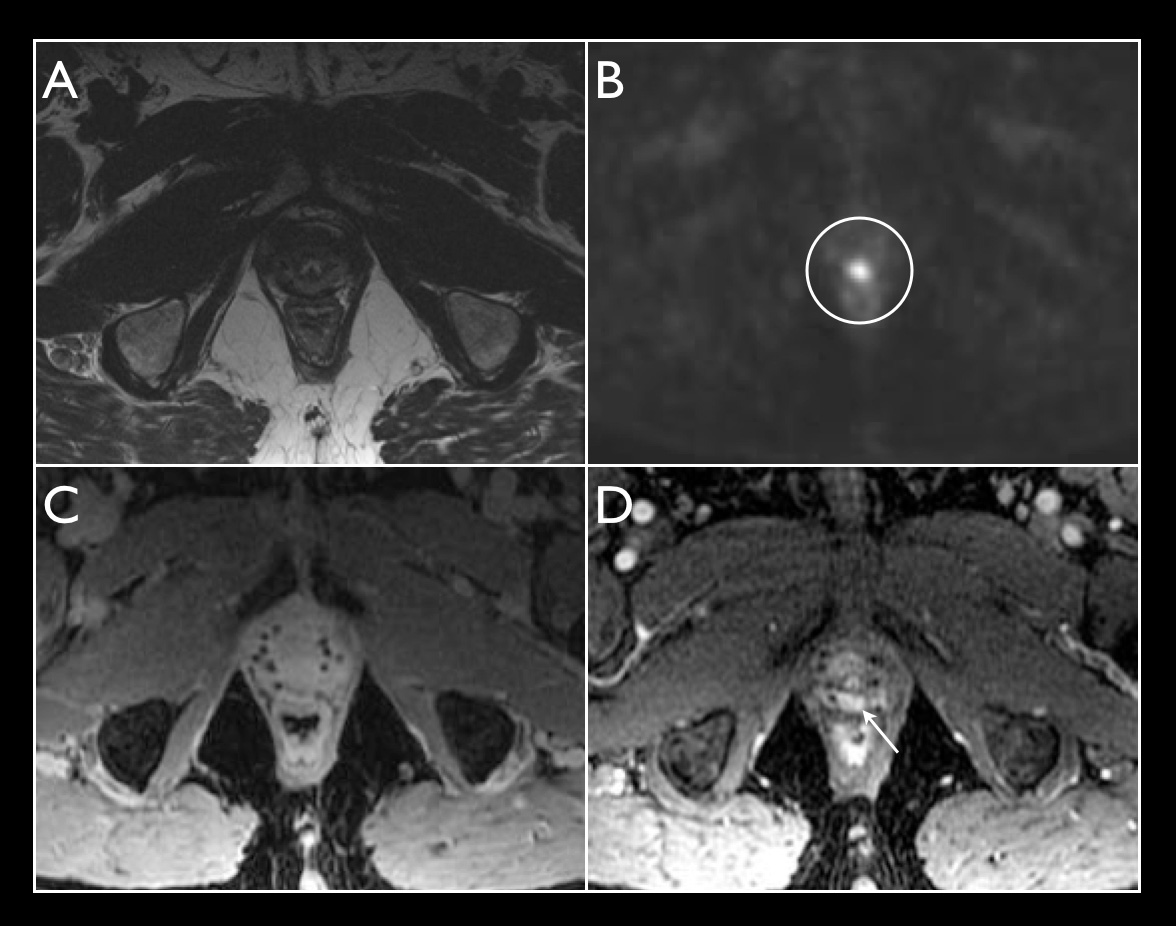
On 68Ga-PSMA-11 PET/MRI for biochemically recurrent prostate cancer, small PSMA-positive lesions are detected on some, but not all MRI sequences. To determine the most effective sequences to obtain for a 68Ga-PSMA-11 PET/MRI protocol, the sensitivities of small FOV T2, T1 post-contrast, and diffusion-weighted sequences for identification of small abdominopelvic nodes were evaluated. In addition, multiphasic contrast-enhanced Differential Subsampling with Cartesian Ordering (DISCO) images were evaluated for detection of prostate bed recurrence. Examination of 48 consecutive patients indicates that small FOV T2 images are most sensitive for small abdominopelvic nodes and DISCO images are most sensitive for prostate bed recurrence.
Purpose
68Ga-PSMA-11 PET is used for the detection of metastatic prostate cancer in patients with biochemical recurrence (BCR). This study assessed the utility of different MRI sequences in detecting anatomic correlates for foci of 68Ga-PSMA-11 uptake on PET/MRI in patients with BCR.Methods
Retrospective analysis was performed by a single reader on 48 consecutive patients with BCR prostate cancer who underwent 68Ga-PSMA-11 PET/MRI on a 3.0T time-of-flight PET/MRI (Signa, GE Healthcare). The acquisition included a two bed-position acquisition of the abdomen and pelvis with 8 minutes of PET acquisition simultaneous with MRI, with subsequent whole body PET imaging with 3 minutes of acquisition per bed position. The detection rate of PSMA-positive lesions in the abdomen and pelvis was evaluated on small FOV T2, whole body T1 fat-saturated post-contrast (LAVA-FLEX), and diffusion weighted imaging (DWI) sequences. For prostate bed recurrences, the detection rate on a time-resolved multiphasic contrast-enhanced sequence (DISCO) was also evaluated.Results
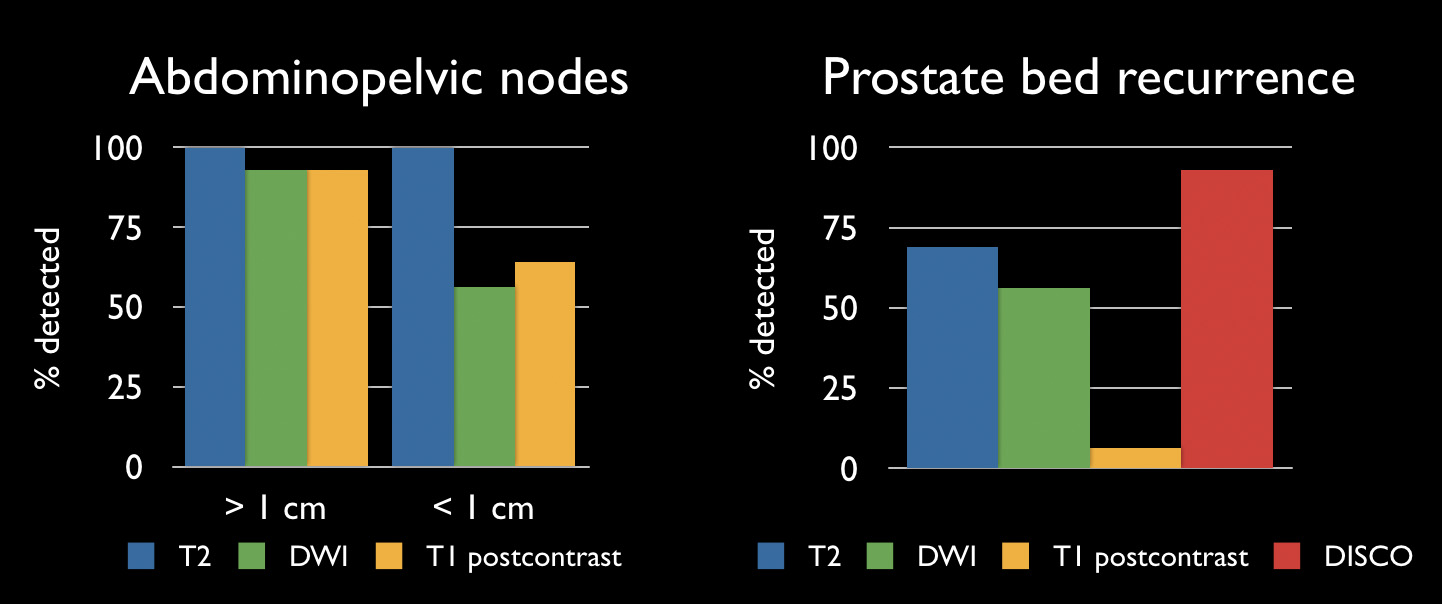
Of the 48 patients, 27.1% had undergone prostatectomy alone, 33.3% had undergone radiation alone (including external beam radiation and/or brachytherapy), and 33.3% had undergone both prostatectomy and radiation. 3 of the patients had undergone other treatments, such as androgen deprivation therapy. Average PSA at time of PET/MRI was 7.4 ng/mL (range 0.05-45.1 ng/mL). PSMA-positive disease was detected in 40 of 48 patients (83.3%). The overall rate of detection of disease was 62.5% (5 of 8 patients) for PSA between 0 and 1 ng/mL, 70.0% (7 of 10 patients) for PSA between 1 and 2 ng/mL, and 93.3% (28 of 30 patients) for PSA greater than 2 ng/mL. With small FOV T2-weighted images, 14 of 14 (100%) abdominopelvic nodes greater than 1 cm in short axis and 39 of 39 (100%) abdominopelvic nodes less than 1 cm in short axis were detected. LAVA-FLEX detected 13 of 14 (92.9%) nodes greater than 1 cm and 25 of 39 (64.1%) nodes less than 1 cm. DWI detected 13 of 14 (92.9%) nodes greater than 1 cm and 22 of 39 (56.4%) nodes less than 1 cm. Small FOV T2-weighted images detected 11 of 16 (68.8%) prostate bed recurrences. LAVA-FLEX detected 1 of 16 (6.3%) prostate bed recurrences. DWI detected 9 of 16 (56.3%) prostate bed recurrences. DISCO images detected 13 of 14 (92.9%) prostate bed recurrences, with 2 of the 16 patients with prostate bed recurrence not undergoing DISCO imaging.
Conclusions
68Ga-PSMA-11 PET/MRI detected PSMA-positive foci in a high percentage of patients with BCR. Small FOV T2-weighted imaging is more sensitive than LAVA-FLEX or DWI for demonstrating the correlating abdominopelvic nodes less than 1 cm in short axis. DISCO is more sensitive than T2-weighted, LAVA-FLEX, or DWI for prostate bed recurrence, with the limitations likely due to radiation changes in the prostate as well as artifact from brachytherapy seeds.Acknowledgements
No acknowledgement found.References
No reference found.Figures