1313
Rapid continuous multiarterial MRI of the hepatic arterial dominant phase during free-breathing.1Radiology, University Hospital Tübingen, Tübingen, Germany, 2Radiology, University Hospital Tübingen, 3Siemens Healthineers
Synopsis
Acquisition of continuous multiarterial MRI of hepatic arterial dominant phase during free-breathing using a free-breathing self-gated spoiled gradient-echo sequence with compressed sensing is feasible and yields excellent arterial enhancement with good compensation of respiratory artifacts and can improve robustness of arterial Phase liver MRI
Introduction
Arterial phase MRI is recommended in liver MRI guidelines as an important part of multiparametric liver MRI. However, the robustness of this sequence is limited in clinical routine, oftentimes due to inadequate vessel- and lesion contrast (1) as well as breathing artifacts in patients who are unable to hold their breath during Liver MRI (2). We hypothesize that fast multiarterial liver MRI with freebreathing techniques can improve the robustness of arterial phase liver MRI. We therefore aimed to evaluate the feasibility of multiarterial MRI of the hepatic arterial dominant phase (HAD) using a free-breathing self-gated spoiled gradient-echo sequence with compressed sensing (CS).
Methods
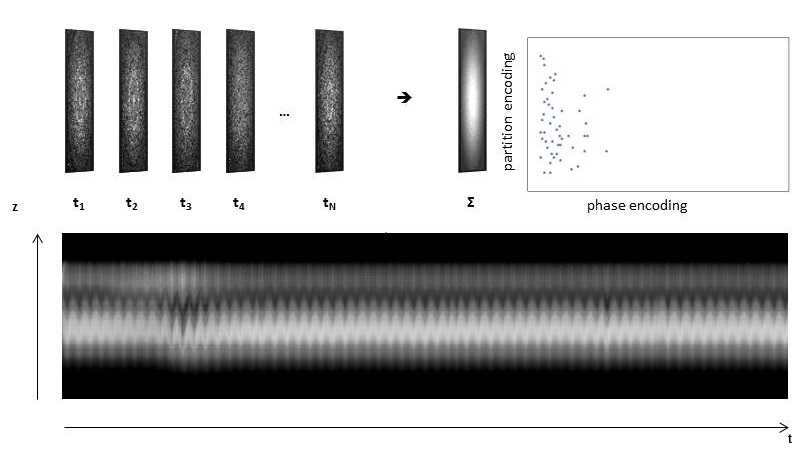
40 patients underwent contrast-enhanced liver MRI with Gadobutrol (Bayer Healthcare). Each 20 patients were examined in 1.5 and 3T (Magnetom Aera and Skyra, Siemens Healthineers), respectively. Multiarterial imaging was performed for 64s beginning with contrast agent injection using a rapid free-breathing prototype volume interpolated breath-hold examination (VIBE)-sequence with CS and automated respiration gating (iVIBE, 1,2x1,2x3mm3), see Figure 1. 8 consecutive subphases were reconstructed (8s/phase). Two independent readers selected and assessed the best HAD phase on a five-point Likert scale (5=excellent) regarding image quality, compensation of respiratory artifacts, enhancement of abdominal aorta and hepatic artery, lesion detectability and diagnostic confidence. Signal intensity (SI) and SNR were measured in the liver and in the abdominal aorta.
Results
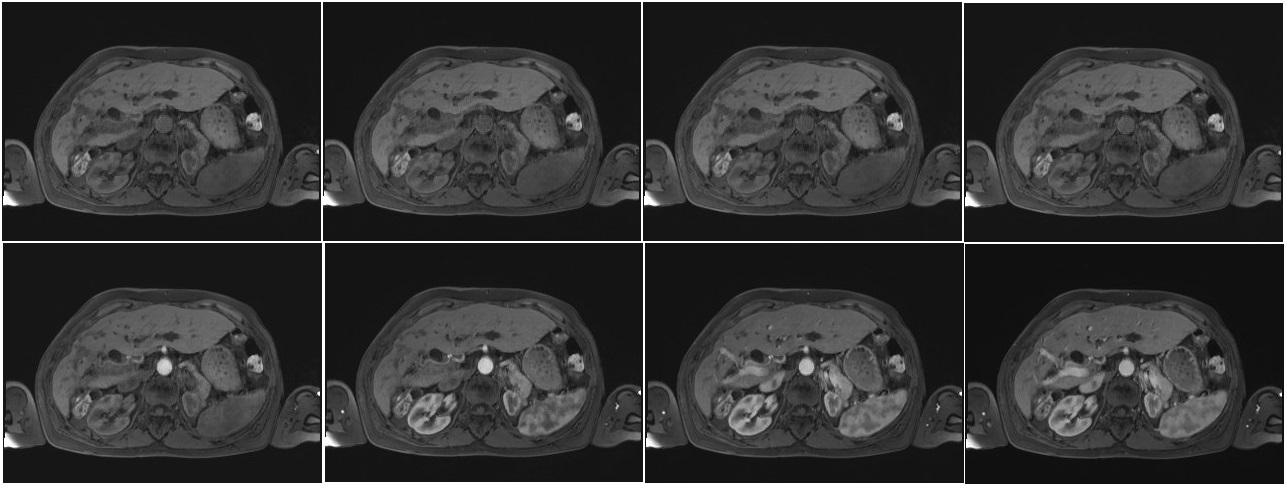
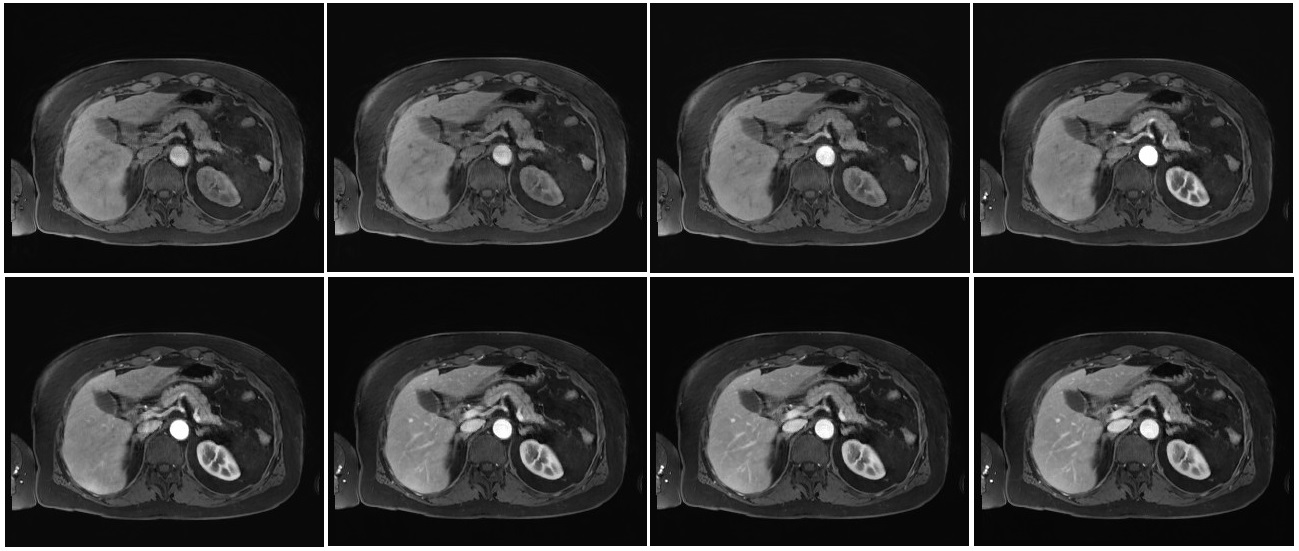
HAD phase varied among patients (3rd – 7th). Image quality and respiratory artifact compensation was rated good (median=4, 3-5) without significant differences between 1.5T and 3T (p≥.089). Lesion detectability, contrast enhancement of aorta and diagnostic confidence were rated excellent (median 5, 3-5) without significant differences among field strengths (p≥.165). Signal intensity and liver SNR were significantly higher in 3T (p≤.015). SNR in the abdominal aorta was high in both field strengths without significant differences (p.=637). Examples of the sequence in both field strengths are given in Figures 2 and 3.
Discussion
The results of this study indicate that multiarterial MRI of the hepatic arterial dominant phase (HAD) using the iVIBE sequence is feasible and leads to a sufficient compensation of respiratory artifacts with excellent arterial contrast in both 1.5T and 3T. Prior studies have shown that multiarterial liver imaging improves arterial contrast and lesion detectability. The use of the proposed multiarterial iVIBE sequence might further improve robustness of arterial liver MRI as it results in good compensation of respiratory artifacts.
Conclusion
Acquisition of continuous multiarterial MRI of hepatic arterial dominant phase during free-breathing using iVIBE is feasible and yields good image quality and excellent arterial enhancement with good compensation of respiratory artifacts resulting in excellent diagnostic confidence in both 1.5T and 3T.
Acknowledgements
NoneReferences
1. Kazmierczak P M, Theisen D, Thierfelder KM et al. Improved Detection of Hypervascular Liver Lesions With CAIPIRINHA–Dixon–TWIST–Volume-Interpolated Breath-Hold Examination. Investigative radiology 2015; 50(3), 153-160.
Figures