1303
High resolution free breathing abdominal imaging1Philips Research Europe, Hamburg, Germany
Synopsis
The scan resolution of abdominal MR imaging using Cartesian sampling is generally limited by the breath-holding capability of the patient, as the respiratory motion would introduce ghosting artefacts. Here we show that golden-angle stack-of-stars sampling in combination with retrospective motion state binning and elastic registration enables sub millimeter in-plane scan resolutions. The technique allows the patient to breathe freely during the examination, hence improving the patient’s comfort, and simultaneously increasing the achievable scan resolution.
Purpose
Magnetic resonance (MR) imaging of large field of views at high spatial resolution results in long acquisition times due to the required matrix size and prolonged sampling time to achieve a sufficient SNR. This is particularly challenging in applications like abdominal imaging, using Cartesian k-space sampling, as the acquisition needs to be completed within a breath-hold to avoid ghosting artefacts due to subject motion. Hence, the acquisition time is limited by the breath hold capability of the patient. Alternatively a radial acquisition scheme may be used. This has more benign motion artefact behavior compared to Cartesian sampling, thus acquisition may be performed during free-breathing and being not limited by not scan time limited. However subject motion during radial acquisition will induce blurring artefacts which are particularly problematic at high resolutions. In this study we demonstrate that using a golden angle stack-of-stars sampling scheme[1], combined with individual reconstruction of multiple motion states and subsequent morphing and combining in image space enables sub millimeter in plane resolution.Methods
A 3D stack of stars acquisition was used,
with Cartesian phase encoding in slice (FH) direction and in-plane radial
sampling. A single-echo fat suppressed e-THRIVE sequence was used with
TR = 4.6 ms, TE = 1.8 ms, and 10° flip angle. In vivo
abdominal images were obtained on a Philips Ingenia 3T scanner with a 12 channel posterior and a 16 channel anterior
coil from healthy volunteers, with a FOV of 450 × 450 × 202 mm³ and 0.9 × 0.9 ×
2 mm³ voxel size. Golden angle radial sampling scheme was used where the angle
increment between two successive readouts is given by 111.25°. 1000 profiles
per slice were acquired from free breathing subjects amounting to 3 minutes
total scan time. Images from individual coils were separately gridded and combined
via an optimal Roemer reconstruction taking the receive coil sensitivities into
account. The acquired radial profiles are sorted into four motion states, using
a k0 auto-navigator[2], [3]. Profiles
from each motion state were reconstructed individually. A modified non-rigid,
non-parametric registration method consisting of elastic registration steps was
applied to generate motion-corrected images[4], by
deforming the individual motion states onto one reference state. The deformed
images are then combined onto and averaged with the reference image for
increased SNR.Results
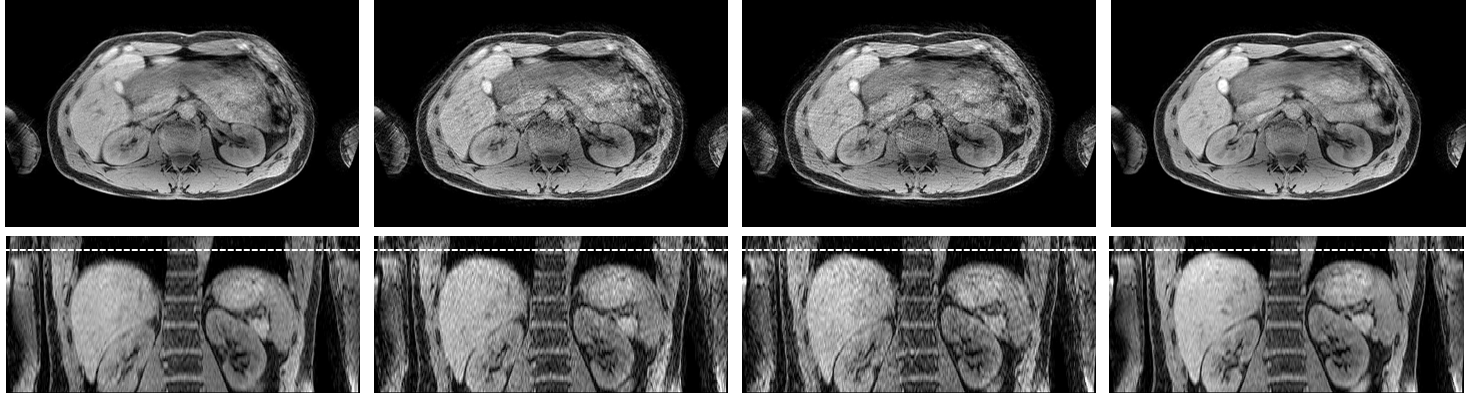
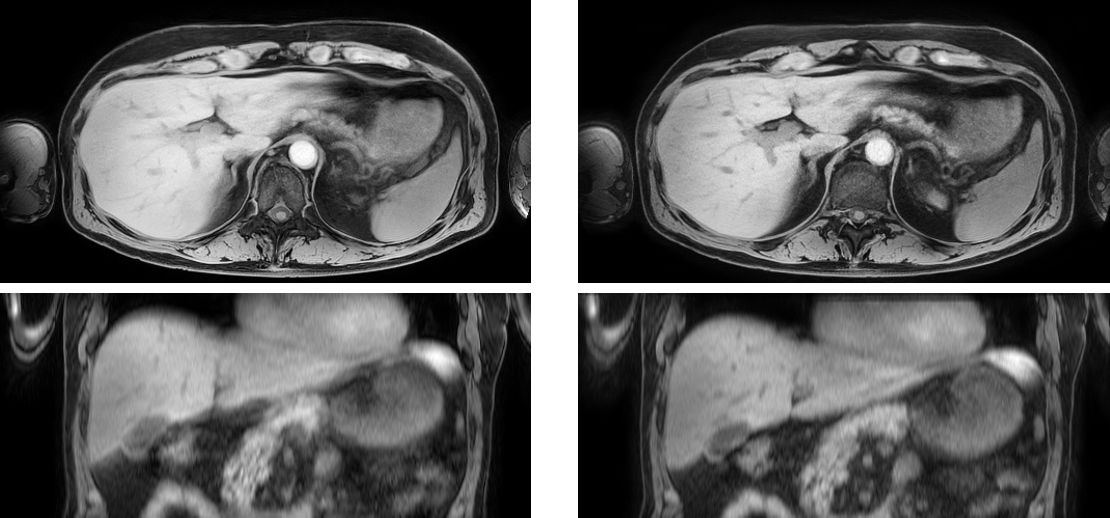
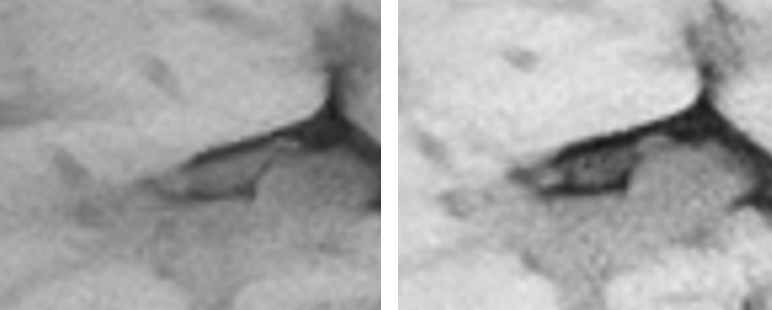
Figure 1 displays the reconstruction results of the individual motion states in axial slice as well as coronal reformat. The translation and deformation of the organs due to respiration is clearly observable. The end inspiration as well as the end expiration state each contain more than 300 profiles, whereas the two other states have less than 200 profiles, resulting in streaking artefacts in the axial slices. The streaking manifests also in the coronal slice, where they appear noise-like. The result of elastic registration, morphing and combination is displayed in the right hand panel of Fig. 2. The blurring is greatly reduced, revealing finer details of the organ structure and increased image sharpness compared to the reconstructed image using all profiles (left in Fig. 2, magnification shown in Fig. 3).Discussion
The golden angle stack-of-stars acquisition combined with auto-navigated multi-bin reconstruction and subsequent image deformation enables imaging resolution not achievable with Cartesian trajectories. This would allow detection of even very small lesions, while at the same time increasing the patient comfort. The presented method may be further refined, by separating the profiles into more than four motion states or even including cardiac motion into the binning process.Acknowledgements
No acknowledgement found.References
[1] S. Winkelmann, T. Schaeffter, T. Koehler, H. Eggers, and O. Doessel, “An Optimal Radial Profile Order Based on the Golden Ratio for Time-Resolved MRI,” IEEE Trans. Med. Imaging, vol. 26, no. 1, pp. 68–76, Jan. 2007.
[2] T. Schäffter, V. Rasche, and I. C. Carlsen, “Motion compensated projection reconstruction,” Magn. Reson. Med., vol. 41, no. 5, pp. 954–963, May 1999.
[3] A. C. Larson et al., “Preliminary investigation of respiratory self-gating for free-breathing segmented cine MRI,” Magn. Reson. Med., vol. 53, no. 1, pp. 159–168, Jan. 2005.
[4] S. Kabus and C. Lorenz, “Fast elastic image registration,” in Medical Image Analysis For The Clinic - A Grand Challenge, 2010, pp. 81–89.
Figures