1279
Gating PET data for cardiac imaging with radial MRI data1Department of Clinical Radiology, University of Muenster, Muenster, Germany, 2European Institute for Molecular Imaging, University of Muenster, Muenster, Germany, 3Department of Nuclear Medicine, University Hospital Muenster, Muenster, Germany
Synopsis
The increasing availability of MR/PET scanners opens new perspectives for cardiac imaging. However, technical issues for the reconstruction of signal from the moving myocardium remain to be solved. Using the k-space center in radial cardiac MRI data allows for generating a robust gating signal. Here, MR data acquired with a radial FLASH sequence in a 3 T MR/PET scanner continuously during a 15 minutes PET acquisition were used for retrospective gating. The k-space center magnitude was used to sort MRI and PET data into different cardiac phases while respiration-corrupted data were excluded, resulting in well separated cardiac phases.
Purpose
The increasing availability of MR/PET scanners opens new perspectives for cardiac imaging. However, technical issues for the reconstruction of signal from the moving myocardium remain to be solved. Using the k-space center in radial cardiac MRI data allows for generating a robust gating signal. Here, MR data acquired with a radial FLASH sequence in a 3 T MR/PET scanner continuously during a 15 minutes PET acquisition were used for retrospective gating. The k-space center magnitude was used to sort MRI and PET data into different cardiac phases while respiration-corrupted data were excluded, resulting in well separated cardiac phases.Introduction
Hybrid MR/PET scanners have become available in the recent years, and promise novel diagnostic options. With regard to moving organs, such as lung or heart, gating procedures for the acquired PET signal are required. In case of hybrid imaging, MRI data can be used for retrospective gating, instead of conventional devices such as respiratory belts or pillows and ECGs [1], avoiding attenuation effects that may corrupt PET data. For MR-based retrospective gating, radial trajectories are suitable because the k-space center magnitude provides a reliable gating signal. Here, the gating signal, derived from the k-space center magnitude was used to sort the PET data into cardiac phase-specific frames.Methods
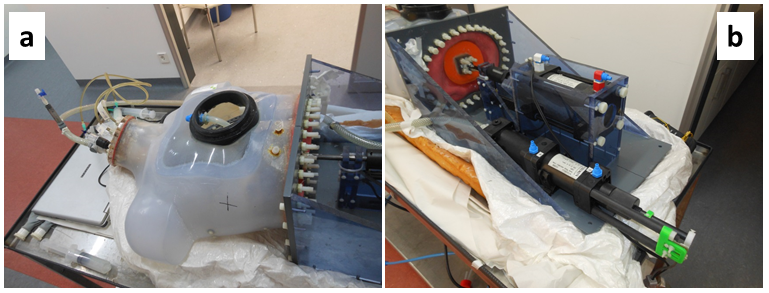
For MR/PET measurements a fully MR-compatible phantom “Wilhelm”, simulating both respiratory and cardiac motions [2], was used (Fig. 1a and b). Periodic motions of Wilhelm were driven by compressed air. Respiratory motion was set to a period of 6 s, cardiac cycle duration was 1 s, mimicking a free breathing patient. All measurements were performed on a 3 tesla MR/PET scanner (Siemens mMR Biograph) using a 32-channel body coil. A radial FLASH sequence (FOV = 300 x 300 mm, slice thickness: 5 mm, Matrix: 128 x 128 and 377 spokes) with golden angle sampling was performed 315 times. The k-space center magnitude of each acquired spoke of the MR data was used to create a gating signal. For derivation of the correct frequencies of cardiac and respiratory cycles, a spectrum was generated by Fourier transformation of the k-space-center magnitudes. After removal of respiration-affected data, the remaining spokes were reordered with respect to the cardiac phase in several frames. Using this signal, the PET data were resorted into 12 frames and merged with the corresponding MR images. For later comparison, additional reference scans without any motion were acquired in systolic and diastolic position of the phantom.Results
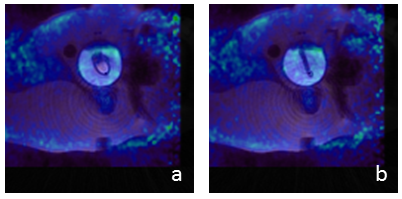
Both respiratory and cardiac motion was visible in the spectrum of the k-space center magnitudes at fresp = 0.167 Hz and fcard = 1 Hz, respectively. The temporal shift between PET and MR acquisition start was calculated as 884 ms by correlation between k-space center magnitudes and the respiration signal from PET counts. During reconstruction of MR data, 45% of all data were rejected because of motion corruption caused by respiration. As a consequence, each of the 12 reconstructed PET frames contained only data of 41 s of PET acquisition (Fig. 2a). Different phases of cardiac motion were resolved in the images as shown by comparison with the reference images acquired without any motion (Fig. 2b) and lower activity in the gated images resulted from the longer scan time of 8 min each of the reference images. The reference image in diastole (Fig. 2b) corresponds to frame 3 and the systolic reference (Fig. 2c) corresponds to frame 9. Overlay of these two frames with MRI is shown in Fig. 3.Discussion
MR data were successfully used to gate the PET data. K-space center magnitude allows for deriving a reliable gating signal for PET and MRI data simultaneously, without using additional attenuating devices or requiring breath-hold. With longer acquisition duration in favor of higher PET contrast, self-gated cardiac MR/PET with radial trajectories may become a powerful tool in imaging cardiac diseases.Acknowledgements
No acknowledgement found.References
[1] Judenhofer MS et al. Applications for Preclinical PET/MRI. Semin Nucl Med 2013; (43): 19-29
[2] Fieseler M et al. A dynamic thorax phantom for the assessment of cardiac and respiratory motion correction in PET/MRI: A preliminary evaluation. Nucl. Inst. and Meth. in Physics and Research A 2015; (702): 59-63
Figures