1264
Highly accelerated Multi-Directional Velocity Encoding 4D Flow MRI: feasibility and preliminary results1Department of Radiology and Biomedical Imaging, University of California, San Francisco, San Francisco, CA, United States, 2Veteran Affairs Medical Center, San Francisco, CA, United States
Synopsis
Velocity-to-noise ratio in 4D flow improves with low velocity encoding (VENC), but is usually compromised to prevent velocity aliasing. Dual-VENC and multi-directional velocity encoding schemes have been proposed to circumvent these issues, but result in an increased acquisition time. In this study, we developed a motion-robust highly accelerated 4D flow acquisition with multi-directional velocity encodings to target applications with a wide range of velocities in clinically acceptable acquisition times, for applications such as imaging of abdominal aneurysms, and simultaneous assessment of cardiac tissue phase mapping and intracardiac blood flow.
Introduction
4D flow MRI provides a comprehensive volumetric coverage of the hemodynamics and allows for a posteriori analyses which can be especially helpful for complicated geometries. Some of the challenges limiting its use in the clinic include: long acquisition times, breathing motion artifacts, and a limited dynamic range of velocities which can be acquired with high velocity-to-noise ratio (VNR). In this study we developed a highly accelerated 4D flow MRI acquisition with multi-directional velocity encodings, targeting clinically acceptable acquisition time, robustness to motion, and an increased dynamic range of velocities acquired with high VNR. The proposed method was tested for imaging of abdominal aortic aneurysm (AAA), a pathology resulting in regions with both low and high blood velocities, as well as imaging of the heart, including both the slower moving myocardium and the faster moving ventricular blood. Our promising preliminary results demonstrated the feasibility of using highly accelerated multi-directional velocity encoding 4D flow MRI in vivo.
Methods
A non-orthogonal encoding scheme using the direction of the vertices of an icosahedron 6, termed ICOSA6, to extend the velocity range outside the prescribed VENC has been shown to improve the VNR ~1.7 times compared to dual-VENC methods1. 4D flow with ICOSA6 encoding has further been exploited to improve the assessment of turbulence2,3. ICOSA6 encoding increases the acquisition time, resulting in acquisition times 1.75 times longer compared to conventional encoding, making acceleration increasingly important for its practical use. Highly accelerated 4D flow MRI based on the CIRcular Cartesian UnderSampling (CIRCUS) strategy4 and combined parallel imaging and compressed sensing reconstruction 5,6 has previously enabled intracranial aneurysm flow imaging in a short scan time of 5 mins with high temporal resolution of <30ms providing an effective acceleration factor of about R=12 7. In this study, we have implemented a highly accelerated 4D flow MRI sequence with CIRCUS and ICOSA6 encoding to assess the velocity imaging of a broad range of velocities. The proposed method was applied to image abdominal aortic aneurysms (AAA), which contain both low and high blood velocities; as well as cardiac imaging, for simultaneously capturing the slower moving myocardium and the faster moving blood in the heart chambers. Data was acquired on a 3.0T Siemens Skyra scanner with an 18-ch body coil and a 32-ch spine coil. For AAA, the scan settings were: VENC=150cm/s, FOV=280x280mm2, slice thickness=2.2 mm, matrix=128x128x58, FA=8o, TR/TE=5.5/3.3ms; for cardiac: VENC=50cm/s, FOV=32x32cm2, slice thickness=7.0 mm, matrix=128x128x16, FA=6o, TR/TE=6.1/4.0ms. With CIRCUS acquisition, the temporal resolution can be chosen retrospectively. In this study, 7 TRs ~40ms was chosen with acceleration factor of R=8 for the AAA case (16 cardiac phases) and R=6 for the cardiac case (18 cardiac phases). The velocity data was post-processed using an in-house developed toolkit written in python. The processing pipeline included: background offset phase correction to compensate for eddy currents, phase unwrapping, segmentation of the vessel/left ventricle and myocardium, computation of velocities from the phase data1 as well as computation of the relative pressure by solving the Pressure Poisson Equation. Streamlines, velocity vectors, and pressure maps were generated using Paraview.
Results
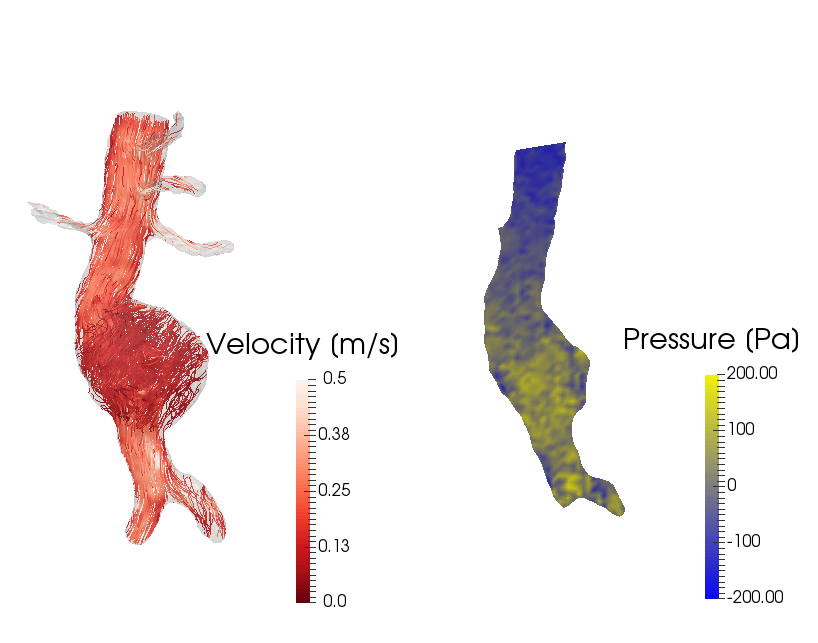
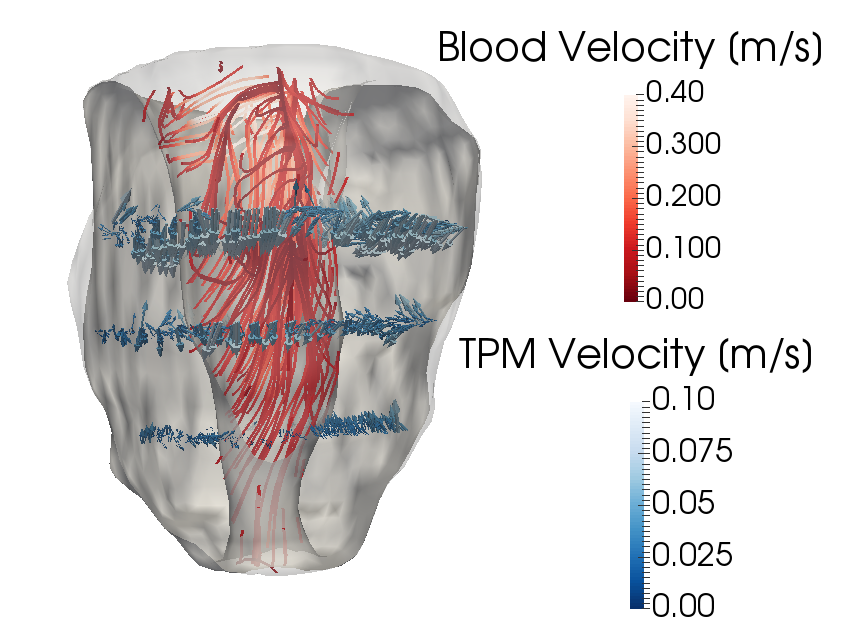
The AAA case required an acquisition time of 10.2 minutes and the results are shown in Figure 1. The figure shows the streamlines in both the high speed tubular lumen and the low speed saccular aneurysm, whereas the pressure map shows the pressure waves arrival at the aneurysm and the iliac bifurcation. The acquisition of the cardiac case required 5.5 minutes and our preliminary results of simultaneously-obtained tissue phase mapping in the myocardium (here displayed in three slices) and intracardial blood flow are shown in Figure 2. The streamlines show the ejection of blood out of the ventricle into the ascending aorta, whereas the arrows show the contraction of the myocardium.
Discussion
This work shows the feasibility of using multi-dimensional 4D flow to assess dynamic flow covering a wide range of velocities. ICOSA6 motion encoding results in a 1.75 longer acquisition time compared to conventional encoding schemes, however, using the CIRCUS undersampling scheme together with compressed sensing and parallel imaging could preserve clinically acceptable acquisition times.
Conclusions
We have implemented and tested a highly accelerated multi-directional velocity encoding 4D flow MRI method for overcoming some of the current technical limitations. Our preliminary results show great potential of the method for applications such as aneurysm and cardiac flow evaluation.
Acknowledgements
NIH K25 EB014914 (JL), NIH R56HL133663 (JL), NIH R01 NS059944 (DS), VA MERIT Review grant (DS).References
1. Zwart NR, Pipe JG. Multidirectional high-moment encoding in phase contrast MRI. Magn Reson Med. 2013;69(6):1553-64. doi: 10.1002/mrm.24390. PubMed PMID: 22760964.
2. Haraldsson H, Kefayati S, Casas B, Lantz J, Ebbers T, Saloner D. Improved full turbulence tensor quantification using ICOSA6 flow encoding for phase-contrast MRI. In: Proceedings of the 23rd Annual Meeting of ISMRM, Toronto, Canada. 2015:2752.
3. Haraldsson H, Kefayati S, Dyverfeldt P, Casas B, Lantz J, Ebbers T, et al. Turbulence Tensor Quantification using ICOSA6 Flow Encoding. Magnetric Resonance Angiography 27th Annual International Conference. 2015:20.
4. Liu J, Saloner D. Accelerated MRI with CIRcular Cartesian UnderSampling (CIRCUS): a variable density Cartesian sampling strategy for compressed sensing and parallel imaging. Quant Imaging Med Surg. 2014 Feb; 4(1):57-67.
5. Otazo R, Kim D, Axel L, Sodickson DK. Combination of compressed sensing and parallel imaging for highly accelerated first-pass cardiac perfusion MRI. Magn Reson Med. 2010;64(3):767-76. Epub 2010/06/11. doi: 10.1002/mrm.22463. PubMed PMID: 20535813; PubMed Central PMCID: PMC2932824.
6. Feng L, Srichai MB, Lim RP, Harrison A, King W, Adluru G, Dibella EV, Sodickson DK, Otazo R, Kim D. Highly accelerated real-time cardiac cine MRI using k-t SPARSE-SENSE. Magn Reson Med. 2013;70(1):64-74. doi: 10.1002/mrm.24440. PubMed PMID: 22887290; PubMed Central PMCID: PMC3504620.
7. Liu J, Koskas L, Faraji F, Kao E, Wang Y, Haraldsson H, Kefayati S, Ahn Sinyeob, Laub G, Saloner D. Highly Accelerated 4D Flow for Intracranial Aneurysm Imaging. ISMRM Workshop on Quantitative MR Flow, San Francisco, Oct 2016.
Figures