1241
Acquisition of sensorimotor fMRI under general anaesthesia in neurosurgical patients: evaluation of the effect of anaesthesia on the BOLD response.1Department of Brain Repair and Rehabilitation, UCL Institute of Neurology, London, United Kingdom, 2UCL Psychology and Language Sciences, Birkbeck-UCL Centre for Neuroimaging, London, United Kingdom, 3Lysholm Department of Neuroradiology, National Hospital for Neurology and Neurosurgery, London, United Kingdom, 4Medical Physics and Biomedical Engineering, University College London Hospital, London, United Kingdom, 5Department of Neurosurgery, National Hospital for Neurology and Neurosurgery, London, United Kingdom, 6Department of Neuroanaesthesia, National Hospital for Neurology and Neurosurgery, London, United Kingdom, 7Department of Neuroanaesthesia and Neurocritical Care, National Hospital for Neurology and Neurosurgery, London, United Kingdom, 8Department of Neurophysics, Max Planck Institute for Human Cognitive and Brain Sciences, Leipzig, Germany
Synopsis
fMRI performed intra-operatively has the potential to significantly improve the outcomes from neurosurgery. The question remains however as to whether the BOLD signal can be detected in anaesthetised patients and what effect anaesthesia has on the response. In 5 patients with brain tumours anaesthetised for surgery we performed a passive sensorimotor fMRI paradigm. Anaesthesia resulted in a reduction in the BOLD response relative to the awake state, but also reduced the variance in the statistical model resulting in significant, accurate activation in all patients.
We conclude that the fMRI BOLD signal can be accurately detected in anaesthetised neurosurgical patients.
Purpose
Accurate localisation of functionally important brain areas is a prerequisite for brain tumour resection to limit post-operative neurological deficits. This has previously been achieved by using pre-operative fMRI or direct intra-operative cortical mapping. Both these techniques have their limitations and challenges. With the increasing prevalence of intra-operative MRI systems within neurosurgical centres, intra-operative fMRI has the potential to become the third major option to guide neurosurgery.
To achieve this, the effect that anaesthesia administered during the procedure to keep the patient unconscious has on the fMRI BOLD signal needs to be investigated. Specifically, it is unclear whether a clinical level of anaesthesia suppresses neural activity and modifies neurovascular coupling to an extent which prevents detection of the BOLD signal. The aim of this study was 1) to determine if sensorimotor fMRI could be acquired under general anaesthesia and 2) to assess the effect of the anaesthesia on the BOLD response.
Methods
With ethical committee approval 5 adult patients with gliomas in the right cerebral hemisphere underwent resection of their tumours in a neurosurgical suite equipped with a 1.5T intra-operative MRI Siemens Espree system. A passive finger flexion sensorimotor fMRI paradigm was performed on both hands1 with the patients firstly awake and then immediately after the induction of general anaesthesia prior to surgery. The clinical depth of anaesthesia was confirmed using a processed EEG based system.
Functional images consisted of a gradient-echo EPI sequence with voxel size of 3 x 3 x 3mm3 (TR/TE/excitation flip angle = 3100ms/40ms/90°), field of view = 192 x 192mm2, 104 volumes of a 42 slice whole brain acquisition. For anatomical reference, a 3D MPRAGE T1-weighted structural image was acquired.
Preprocessing, including normalisation, and the statistical analysis of the fMRI data were performed in SPM12. The data were analysed using a subject specific fixed effect analysis using the GLM2. In the awake state, the largest cluster and location of peak voxel activation for the task at a threshold of p<0.05 after family wise error correction across the whole brain were reported. In the anaesthetised state the threshold was set at an uncorrected level of p<0.001.
The BOLD signal change elicited by the task versus rest was averaged across all the voxels contained within the largest cluster of activation in the awake state using the MarsBaR3 toolbox for SPM. This was repeated in the anaesthetised state. The effect of anaesthesia on the variance across the entire brain within the fMRI 1st level analysis was also calculated for each patient using the ResMS image from the awake and anaesthetised states. Statistical comparison was performed with the Wilcoxon Signed Rank Test in SPSS.
Results
In all patients under general anaesthesia, activation was localised to the expected somatotopic region of the sensorimotor cortex in both cerebral hemispheres with and without the tumour (Figure 1).
The median BOLD signal change from baseline, elicited by the task in the tumoural hemisphere was 1.16% when awake compared with 0.28% under anaesthesia (p=0.04). In the non-tumoural hemisphere BOLD activation was 0.9% when awake compared with 0.17% under anaesthesia (p=0.04) (Figure 2).
The voxel variance in the statistical model across the whole brain in the awake and the anaesthetised state was also reduced from a median group value of 2.2 (awake) to 1.33 (anaesthesia) (p=0.043).
Discussion
The first aim of this study was to determine if BOLD activation in the sensorimotor cortex could be detected in anaesthetised neurosurgical patients prior to surgery. Using a passive finger flexion fMRI paradigm, BOLD activation was accurately elicited in the sensorimotor cortex under anaesthesia in both cerebral hemispheres in all patients.
The second aim was to determine the effect of anaesthesia on the BOLD response. Anaesthesia resulted in a significant reduction in the BOLD response compared to the awake state. We have shown that the variance across the whole brain measured in the 1st level statistical model was also reduced by anaesthesia. We propose that a global reduction in brain activity, induced by the state of unconsciousness from anaesthesia, results in a reduction in the unexplained voxel variance, and allows for significant task related activation despite a large reduction in the BOLD signal. These results provide insight into the effect of anaesthesia on neurovascular coupling within the brain.
Conclusion
This study demonstrates that sensorimotor fMRI can be acquired under general anaesthesia and is the first step in the realisation of intra-operative fMRI as a method for neurosurgical guidance.Acknowledgements
No acknowledgement found.References
1. Magerkurth J, Mancini L, Penny W, Flandin G, Ashburner J, Micallef C, et al. Objective Bayesian fMRI analysis-a pilot study in different clinical environments. Front Neurosci 9:1–17, 2015
2. Friston KJ, Ashburner JT, Kiebel SJ, Nichols TE, Penny WD (eds): Statistical Parametric Mapping. The Analysis of Functional Brain Images. Academic Press, 2006
3. Brett M, Anton JL, Valabregue R, Poline JB: Region of interest analysis using an SPM toolbox, in 8th International Conference on Functional Mapping of the Human Brain. 2002
Figures
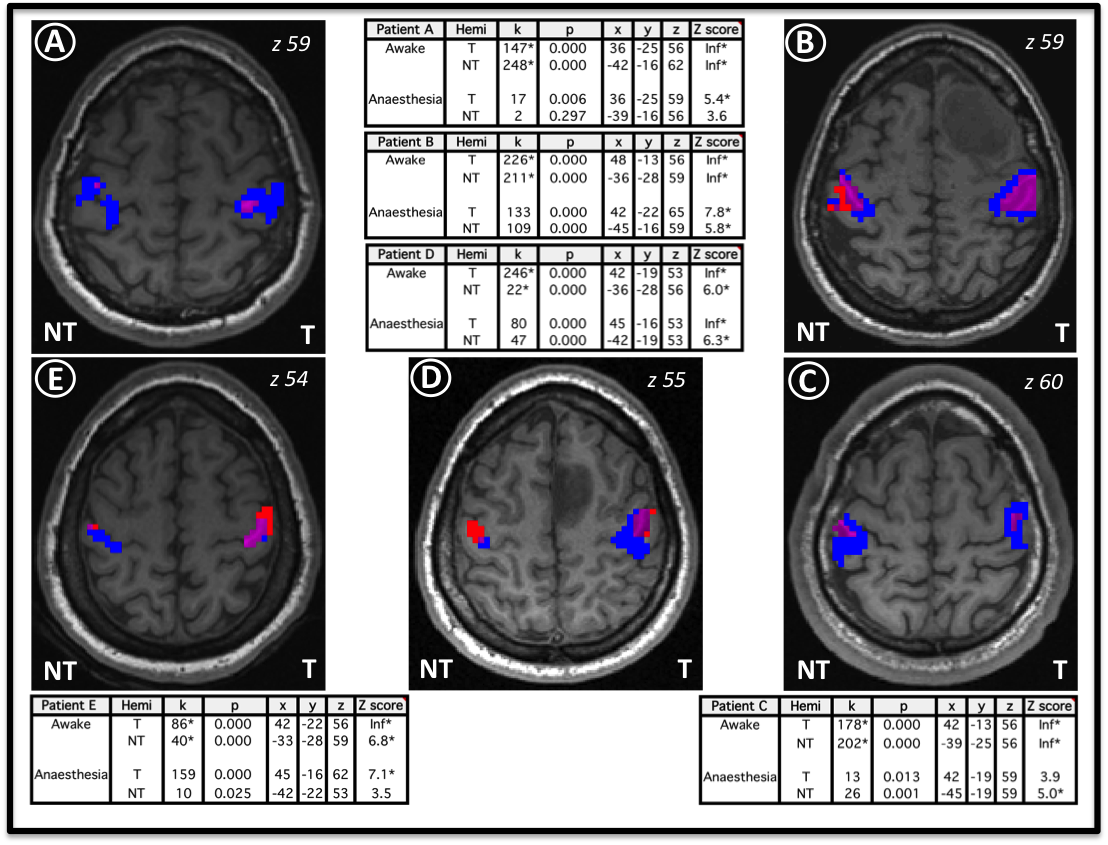
Figure 1
Illustrates the fMRI activation clusters on T1 weighted slices in neurological convention for the left hand (T= tumoural hemisphere) and right hand (NT= non tumoural hemisphere) for patients A to E. Blue voxels represent areas of activation seen only in the awake state, red voxels only in the anaesthetised state and purple voxels in both. Tables show the corresponding statistical results.
k = cluster size, p = cluster extent p value, x y z = MNI co-ordinates for peak activation, Z score for peak voxel activation (* p < 0.05 after family wise error correction for multiple comparisons).
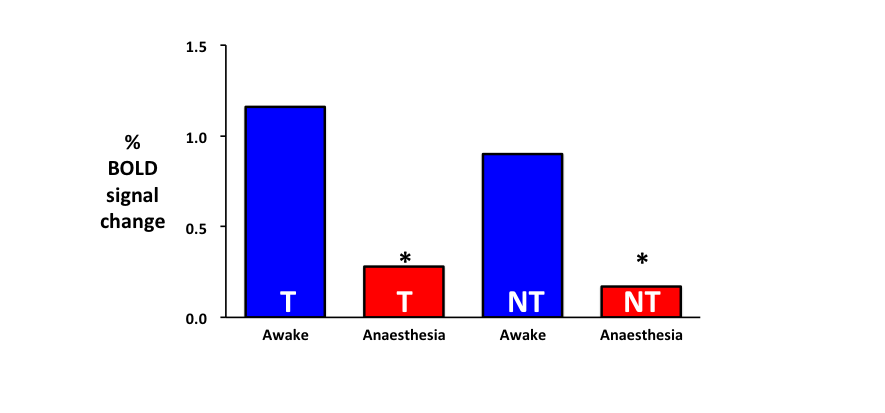
Figure 2
Illustrates the median BOLD signal change from rest elicited by the fMRI paradigm when the patients were awake and when under anaesthesia. T (tumoural hemisphere) represents the activation in the sensorimotor cortex on the same side as the tumour (left hand) and NT (non tumoural hemisphere) represents the activation in the sensorimotor cortex on the opposite side of the tumour. * indicates that the difference was statistically significant (p < 0.05).