1219
A 32-channel transmit system add-on for 7 Tesla body imaging1Erwin L. Hahn Institute for MRI, University Duisburg-Essen, Essen, Germany, 2Medical Physics in Radiology, German Cancer Research Center (DKFZ), Heidelberg, Germany, 3High-Field and Hybrid MR Imaging, University Hospital Essen, Essen, Germany, 4RF & Microwave Technology, University Duisburg-Essen, Duisburg, Germany
Synopsis
At ultra-high field, severe transmit field inhomogeneities affect the quality of imaging. To cope with this, multi-channel solutions are necessary. In this work we present an add-on 32-channel transmit system including an integrated transmit/receive body coil for large field of view imaging. First phantom and in-vivo results are shown. A 50 cm field of view can be achieved and the system is capable of 100 kHz sampling, allowing parallel spatially selective transmit pulses for in-vivo imaging.
Purpose
At ultra-high field, severe excitation inhomogeneities affect the quality of imaging when using volume coils for transmission, which is standard at lower field strengths. In an effort to cope with these problems, multi-channel methods have been developed that statically (RF shimming), semi-dynamically (spokes, k-t-points, TIAMO), or dynamically (Transmit Sense) modulate the amplitude and phase of input signals for multi-channel transmit arrays. To make use of these methods, suitable hardware is a prerequisite. Here we present a 32-channel transmit system as an add-on to a commercial 7 Tesla MRI (Magnetom 7T, Siemens Healthcare, Erlangen, Germany).Methods
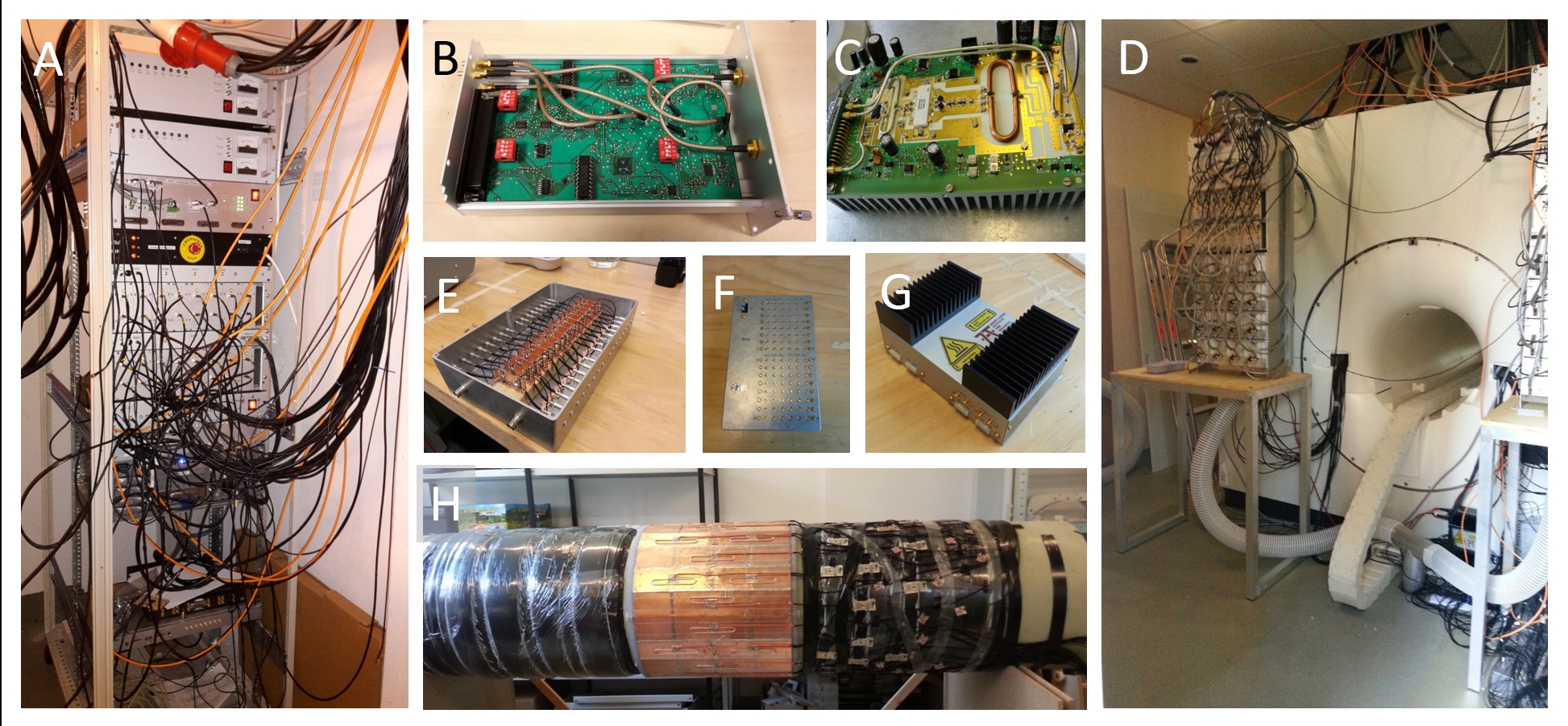
Figure 1 shows a simplified overview of the add-on system, while figure 2 shows photos of some of the components.
The add-on system requires only one analog and three digital input signals from the vendor-provided MRI system. It receives the unblank signal and the T/R signal from the state controller to switch into the correct state, the single-channel RF pulse from the system’s exciter, and a digital trigger from the sequence to set the modulators. Furthermore, the add-on system feeds back received signals from either the transmit coil or dedicated receive coils as well as transmit pulse supervision signals to the original system receivers. Apart from these interfaces, the systems are independent from one another.
The signal from the MRI system’s master exciter can be switched to the 32-channel system and is then split into 32 channels with equal amplitudes and phases. Each of the 32 signals is then fed to I/Q modulators1. The modulators are programmed by an operating PC and assume a new state on each trigger signal from a running pulse sequence with a sampling rate of up to 100 kHz. The modulated signals are fed into 1 kW LDMOS amplifiers2 situated directly at the magnet. The high-power RF signals are fed through directional couplers. The forward and reflected power are measured with logarithmic amplifiers and sent to a supervision computer. In addition, the forward signal can be fed directly into the receivers for complex pulse supervision. An integrated body coil3 is connected to the high-power output of the directional couplers via T/R switches, so that the body array can be used both as a transmit and receive array. A logic controller dynamically sets the states of the different components with logic implemented in hardware for increased robustness. The system can be run with reception either from the body coil or a local array4.
Via the controller’s software, the add-on system can be switched to an offline state in which it is transparent to the original system. The power amplifiers and receive amplifiers are switched off, all switches are switched to a state where the standard signal paths are adopted, and the body coil is switched to a detuned state.
Results
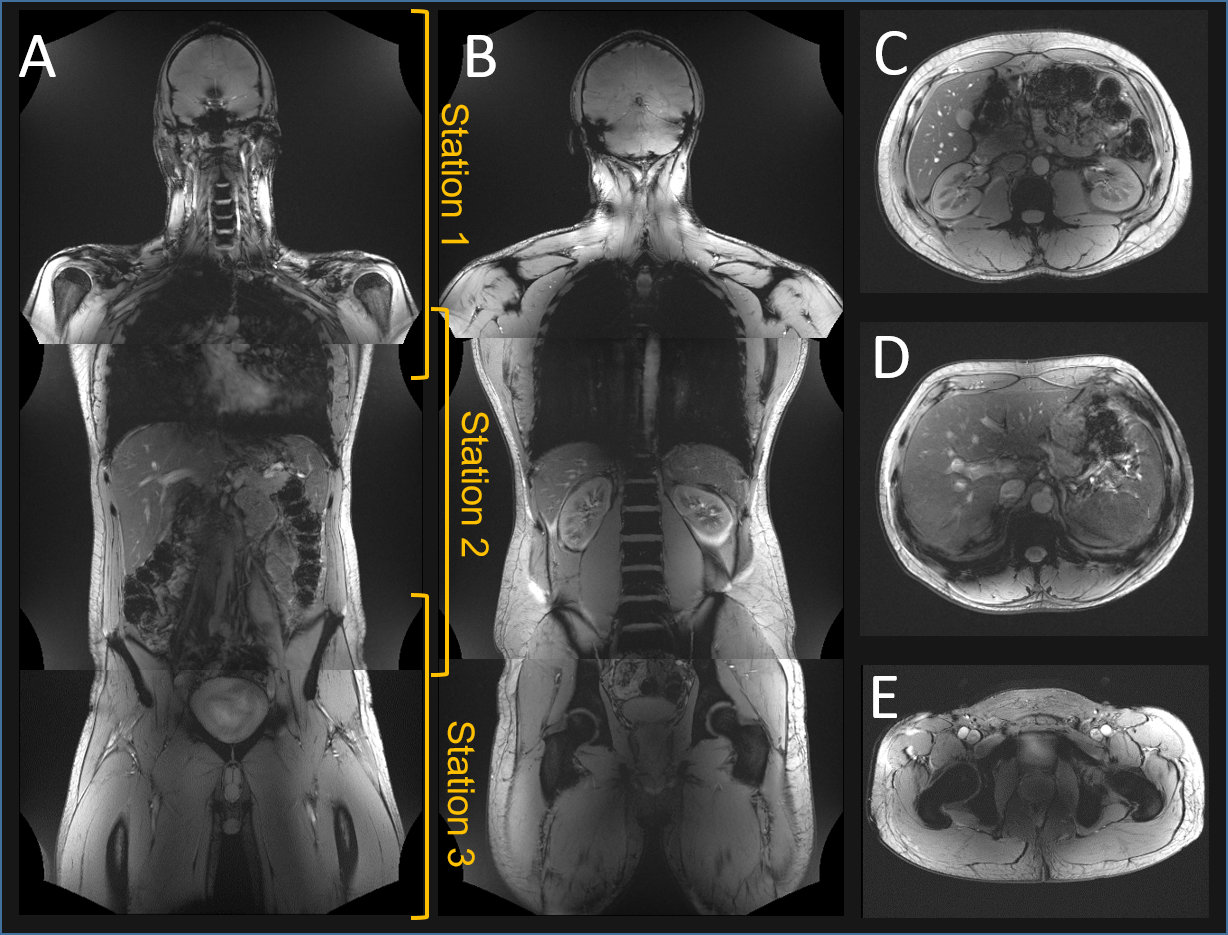
Figure 3 shows a set of images demonstrating first results for large field of view in-vivo body imaging acquired with the 32-channel system in a male volunteer (92 kg, 1.85 m). The head to thigh images (A,B) were acquired in only 3 stations using TIAMO. Each station has a length of 50 cm in the z-direction, and the table was moved by 40 cm between acquisitions. Images C-E show axial slices in different positions. No complete signal dropouts are visible, although only pre-set modes (Cp+ and Cp2+) were used for the TIAMO algorithm.
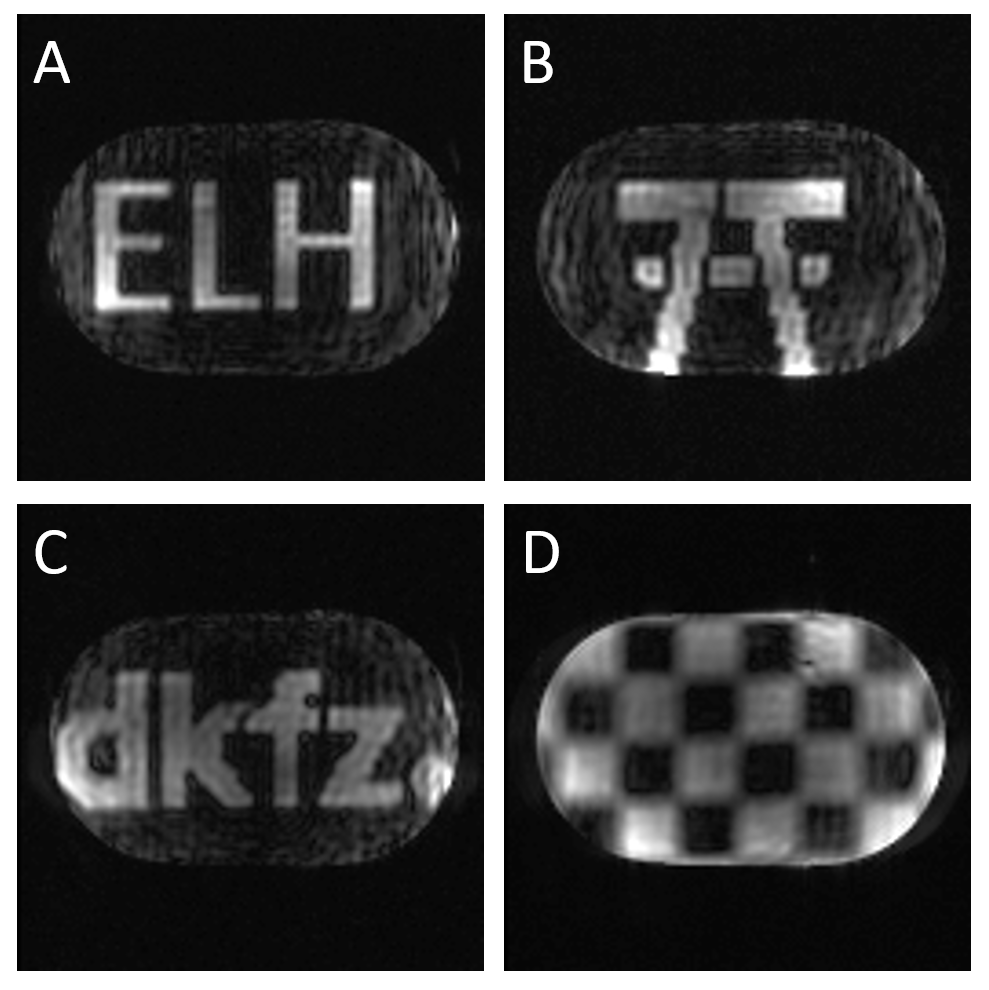
Figure 4 shows 2D spatially selective excitation pTx results from a homogeneous body phantom (340 mm width, 207 mm height, 500 mm length). The integrated body array was used for transmission and reception.
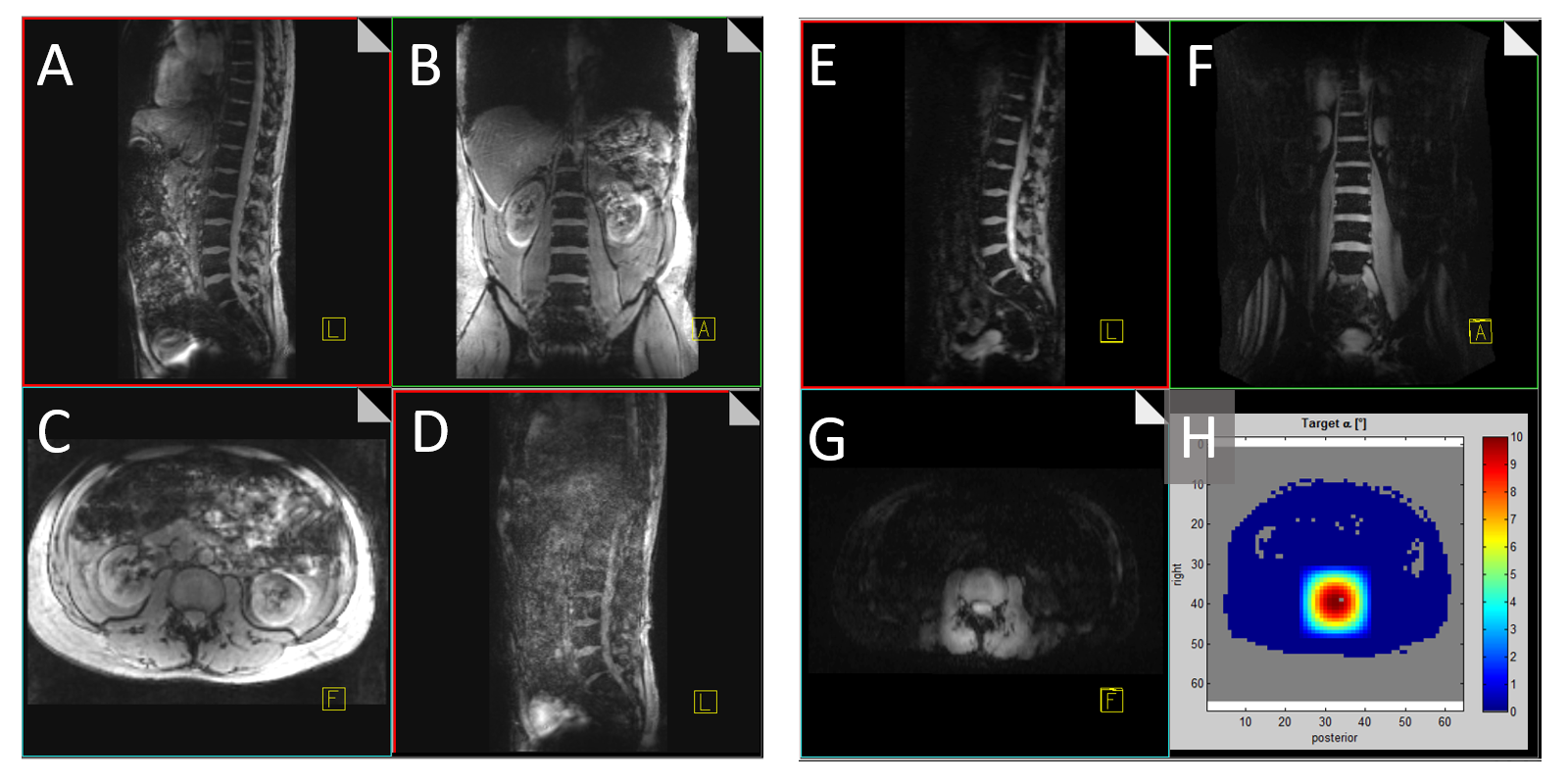
Figure 5 shows the first in vivo full pTx results. A-G show slices from 3D gradient echo data sets. A-C were acquired with TIAMO in breath hold as an anatomical reference. D shows the same sequence acquired during free breathing. E-G show images from a 3D dataset acquired with 2D spatially selective excitation targeted at the spine during free breathing. Very few motion artifacts are visible. H shows the target for the optimization.
QA tests verified that the MRI system works normally when switched back to its original state.
Discussion & Conclusion
First volunteer images show a large field of view of 50 cm with quite homogeneous image intensity. The add-on system enables 32-channel parallel transmit with 10 µs samples over a large field of view as demonstrated in phantoms and in vivo.
Future work will include optimizations of some of the components and further imaging experiments to evaluate the full capabilities of the system.
Acknowledgements
The research leading to these results has received funding from the European Research Council under the European Union's Seventh Framework Programme (FP/2007-2013) / ERC Grant Agreement n. 291903 MRexcite.References
1. Shooshtary S, Gratz M, Ladd M et al. High-Speed RF Modulation System for 32 Parallel Transmission Channels at 7T. Proc. Intl. Soc. Mag. Reson. Med. 2014, p.544.
2. Solbach K, Abuelhaija A, Shooshtary S. Near-Magnet Power Amplifier with Built-In Coil Current Sensing. Proc. Intl. Soc. Mag. Reson. Med. 2014, p.1287.
3. Orzada S, Bitz AK, Solbach K et al. A Receive Chain Add-On for Implementation of a 32-Channel Integrated Tx/Rx Body Coil and Use of Local Receive Arrays at 7 Tesla. Proc. Intl. Soc. Mag. Reson. Med. 2015, p.3134.
4. Orzada S, Bitz AK, Kraff O et al. A 32-Channel Integrated Body Coil for 7 Tesla Whole-Body Imaging. Proc. Intl. Soc. Mag. Reson. Med. 2016, p.167.
Figures