1206
Reconstruction of DCE tracer kinetic parameters from under-sampled data with a flexible model consistency constraint1Electrical Engineering, University of Southern California, Los Angeles, CA, United States
Synopsis
Recently, it has been shown that DCE-MRI tracker-kinetic (TK) parameter maps can be directly estimated from under-sampled (k,t)-space data. Two major limitations of this approach are that 1) the gradient of a complicated cost function with respect to each TK parameter needs to be computed, and 2) it does not allow for any TK model deviation in the data. In this work, we present an alternative formulation where instead of forcing every voxel to follow the selected TK model, the model consistency is used as a constraint with a weighting penalty. This method is uniquely compatible with the use of multiple or nested TK models, and we show that it provides more accurate TK parameter restoration.
Introduction
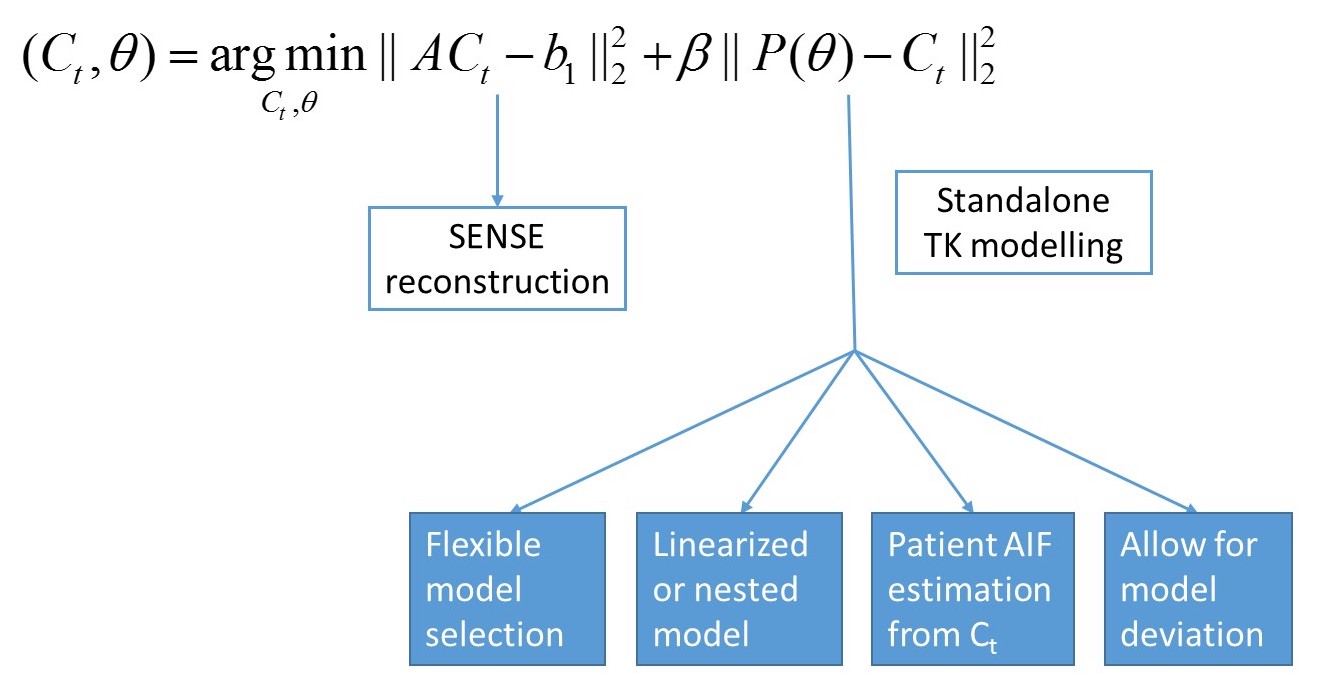
Recently, it has been shown that Dynamic Contrast Enhanced (DCE) MRI tracker-kinetic (TK) parameter maps can be directly estimated from under-sampled (k,t)-space data1,2,3,4. This provided significant improvements in spatial resolution and coverage, and a parameter-free reconstruction3,4. However, this method requires dedicated effort to derive the gradient of the optimization for each different TK model used, and it does not permit any TK model deviation in the data. In this work, we demonstrate an alternative formulation that decouples the reconstruction problem into two simpler parts: 1) SENSE reconstruction, and 2) TK modeling. Similar to recent works in MRI relaxometry5, we utilize TK model consistency as a constraint, and introduces a regularization parameter to weight data and model consistency.Methods
We formulate the DCE reconstruction problem as a penalized optimization problem:
$$(C_t, \theta )= \underset{C_t, \theta}{argmin}||AC_t-b_1||_2^2+ \beta ||P(\theta )-C_t||_2^2\quad (1)$$ where $$$C_t$$$ is the contrast agent concentration over time, and $$$\theta$$$ is the TK parameter maps ($$$K^{trans}$$$, $$$v_p$$$ etc., depending on the TK model), A=UFS$$$\psi$$$ represents under-sampling (U) Fourier transform (F), sensitivity encoding (S) and contrast concentration to image difference conversion ($$$\psi$$$). P represents the forward TK modelling (linear for Patlak, nonlinear for all other TK models). $$$b_1= (y+AS_0)$$$ is the known data, where y is the acquired (k,t)-space data which may be sampled below the Nyquist rate, and $$$S_0$$$ is the fully-sampled pre-contrast image. Note that in contrast to previous direct reconstruction approaches3,4, this formulation allows for penalizing model deviations in the second term, where the regularization parameter $$$\beta$$$ controls the balance between data consistency and model consistency.
To solve the optimization problem in Eqn (1), we alternatively solve for each variable while keeping others constant. For each iteration n:
$$C_t^{n+1}= \underset{C_t}{argmin}||AC_t-b_1||_2^2+ \beta ||P(\theta^n )-C_t||_2^2\quad (2)$$ $$\theta^{n+1}=P^{-1}(C_t^{n+1})\quad (3)$$
Note that Eqn (2) is a SENSE reconstruction that can be solved quickly using conjugate gradients to solve for the concentration vs. time curves ($$$C_t$$$) from under-sampled data, and Eqn (3) is backward TK modelling, which can utilize any DCE-MRI modelling toolbox6. This method essentially decouples data consistency and model consistency, and formulates model consistency as a constraint with a penalty $$$\beta$$$. As illustrated in Figure 1, there are multiple benefits of this new formulation including: 1. reduced computational complexity; 2. flexibility of model selection and linearized/nested models; 3. joint patient-specific AIF estimation; 4. TK model deviation allowed.
We test the proposed method using fully-sampled DCE data sets from brain tumor patients (3T GE MRI, FOV: 22×22cm2, spatial resolution: 0.9×1.3×7.0mm3, 5 s temporal resolution, 50 time frames, fast SPGR). Patient data were retrospectively under-sampled in the $$$k_x-k_y$$$ plane, simulating $$$k_y-k_z$$$ phase encoding in a 3D whole-brain acquisition7, using a randomized golden-angle ratio radial sampling pattern8. Different $$$\beta$$$ values were used to test the influence of model constraint penalties for the reconstruction. After an empirical $$$\beta$$$ value was selected, a broad range of under-sampling rates (R) were used to test the proposed algorithm using Patlak and eTofts model. TK maps from fully-sampled data was considered the reference, and tumor ROI $$$K^{trans}$$$ rMSE and histograms9 were used to evaluate the results.
Results
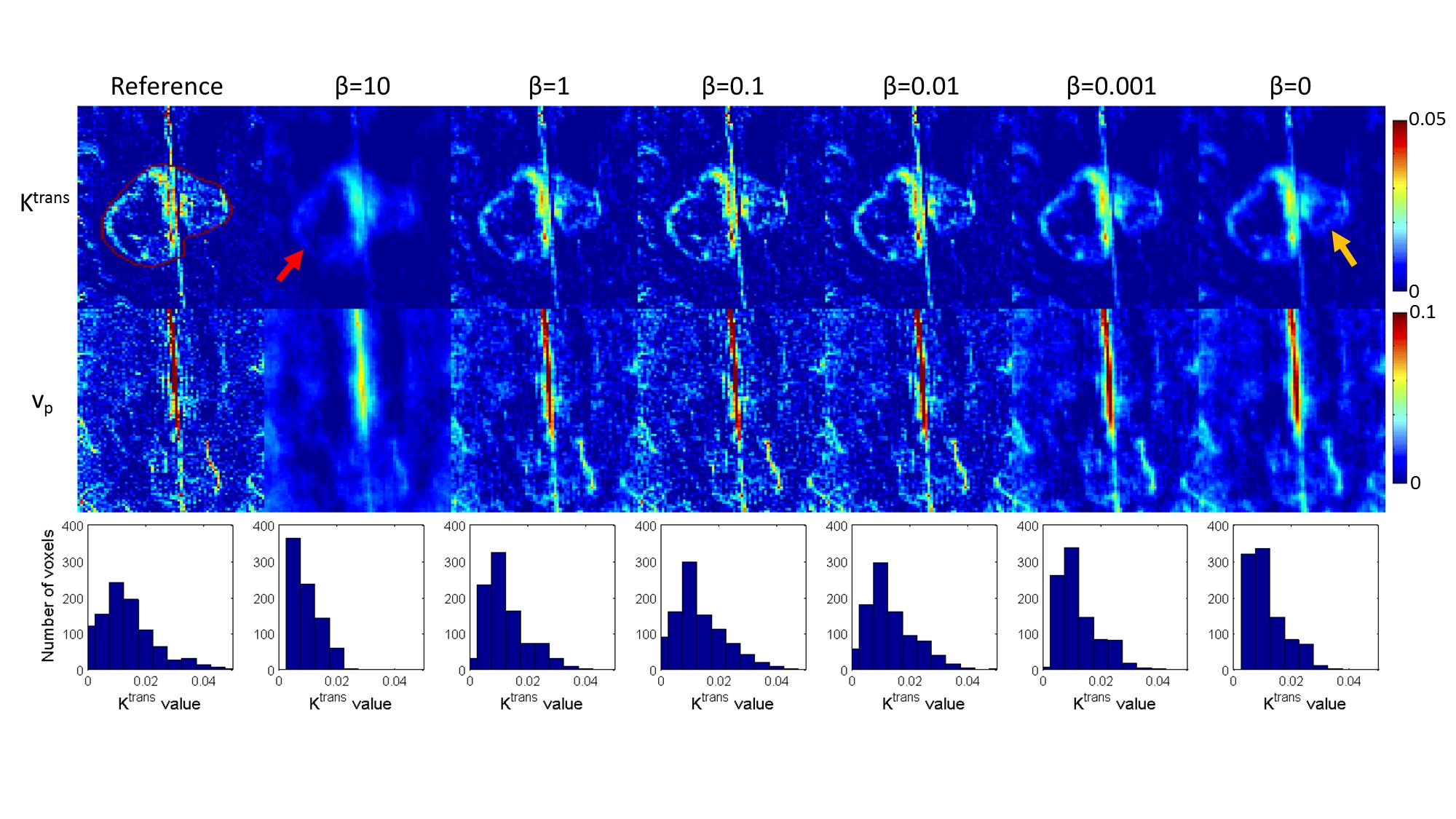
Figure 2 shows results for a broad range of $$$\beta$$$ values. $$$\beta$$$ value within the range 0.01 to 0.1 gave similar results, and a $$$\beta$$$ value of 0.05 was used for further testing.
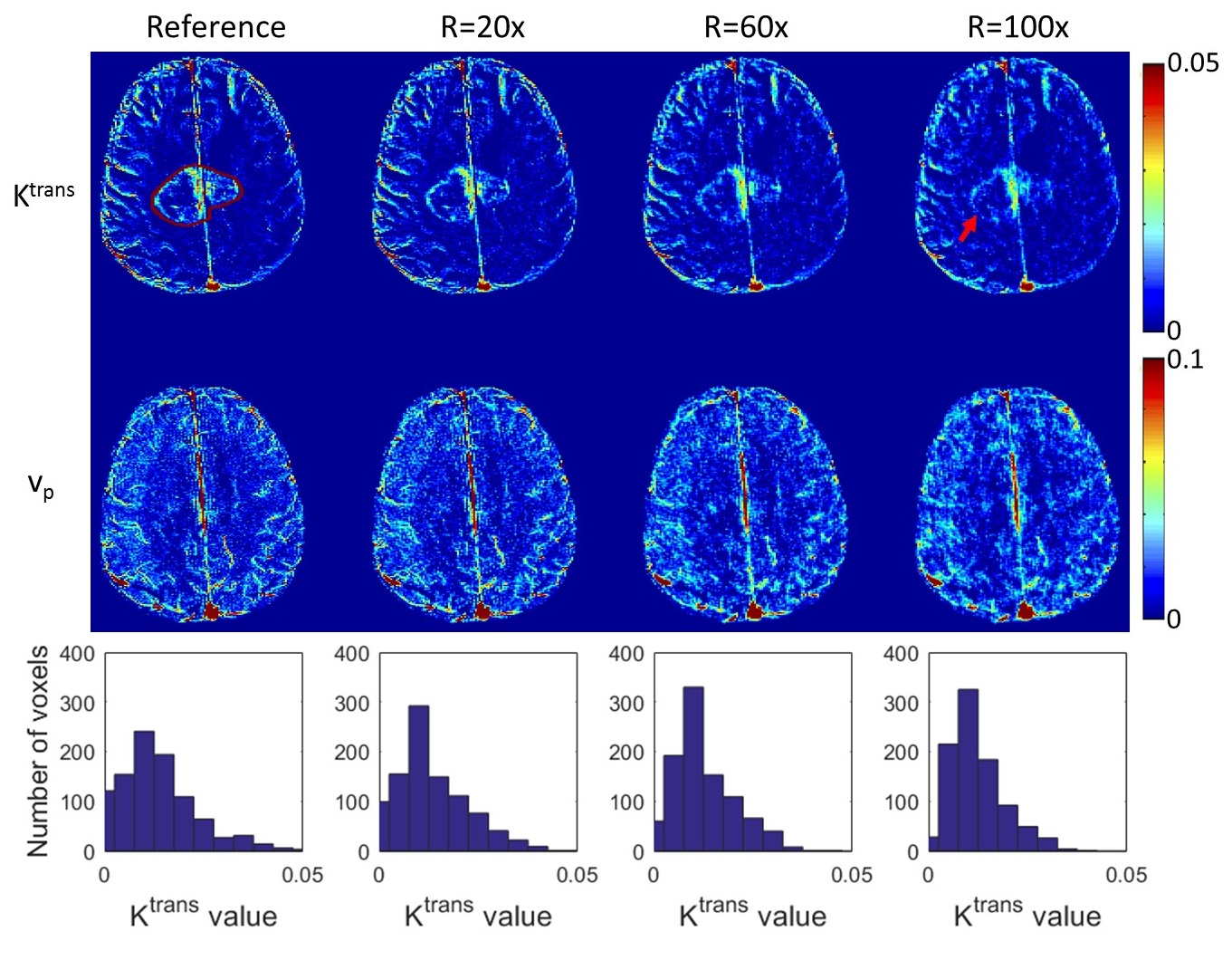
Figure 3 shows $$$K^{trans}, v_p$$$ maps, and $$$K^{trans}$$$ histograms in the tumor ROI (zero values eliminated) from Patlak model at R=20x, 60x, and 100x for the proposed method. Acceptable TK parameter maps were restored at up to R=60x. At R=100x, the degradation of the thin tumor boundary became visually obvious, along with underestimation of $$$K^{trans}$$$ by histogram analysis.
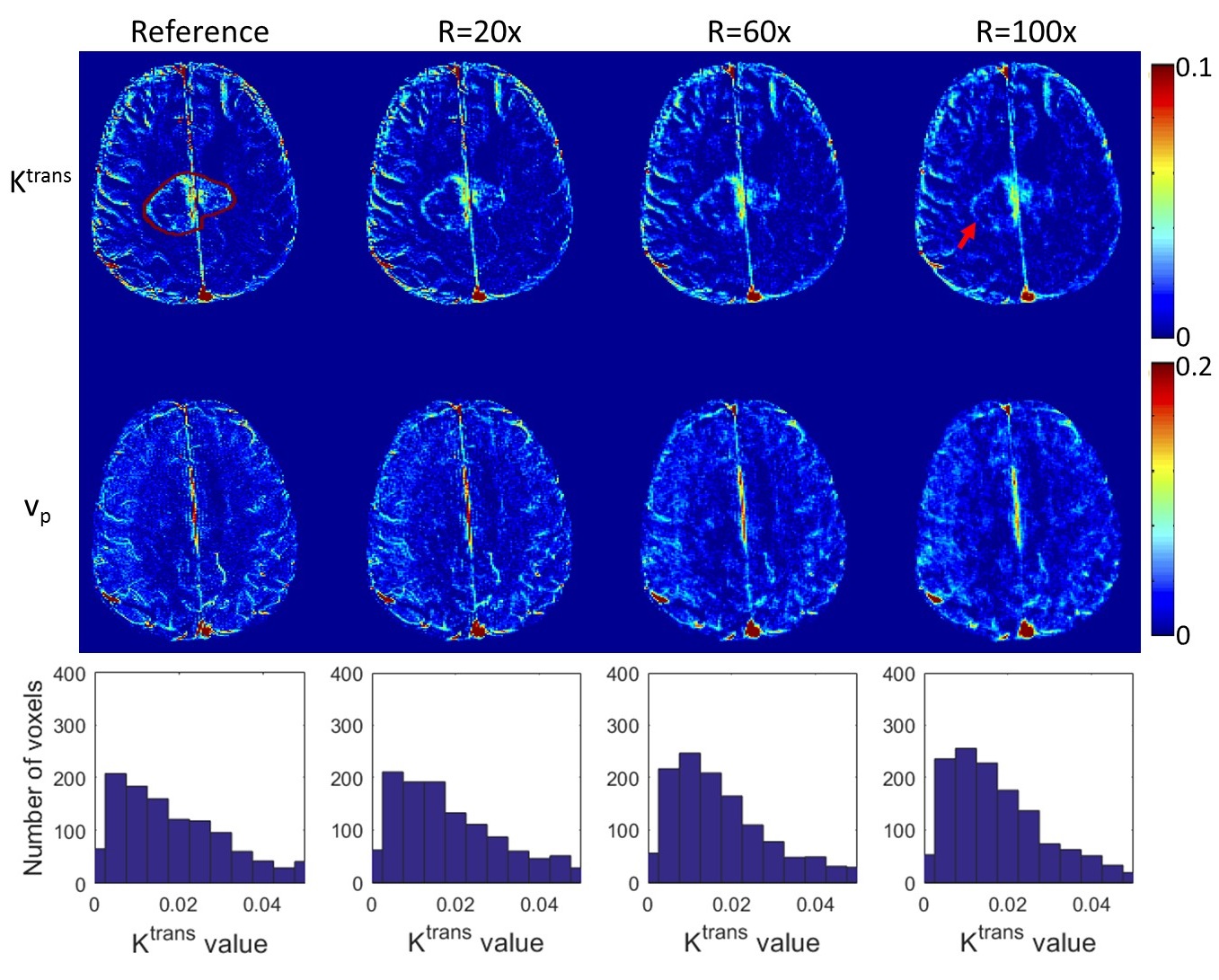
Figure 4 shows reconstruction results for eTofts model at the same undersampling factors. The quality of $$$K_{ep}$$$ maps (not shown) were poor even for fully-sampled data and were therefore not compared. Acceptable quality $$$K^{trans}$$$ and $$$v_p$$$ maps were restored at R=20x, and the quality degrades slightly at R=60x and 100x, based on visual and histogram analysis.
Discussion
We demonstrate a new and flexible approach for accelerated DCE-MRI, where the TK model consistency is applied as a constraint. We demonstrate ease of implementation, and the ability to include non-linear TK models. We demonstrate the use of Patlak and eTofts model, and showed that TK maps can be restored at undersampling rates of up to 60x and 20x, respectively. Although not shown, this framework can be extended to more complex models including nested models, with the possibility to include linearized TK models as an initial step to improve computation time.
Acknowledgements
No acknowledgement found.References
1. Dikaios N, Arridge S, Hamy V, Punwani S, Atkinson D. Direct parametric reconstruction from undersampled (k, t)-space data in dynamic contrast enhanced MRI. Med Image Anal. 2014 May 24;18(7):989–1001.
2. Awate SP, DiBella EVR, Tasdizen T, Whitaker RT. Model-based image reconstruction for dynamic cardiac perfusion MRI from sparse data. IEEE-EMBS, 2006. p.936–41.
3. Guo Y, Lingala SG, Zhu Y, Lebel RM, Nayak KS. Direct Estimation of Tracer-Kinetic Parameter Maps From Highly Undersampled Brain Dynamic Contrast Enhanced MRI. MRM. 2016; (early view)
4. Guo Y, Lingala SG, Zhu Y, Lebel RM, Nayak KS. Direct Reconstruction of Kinetic Parameter Maps in Accelerated Brain DCE-MRI using the Extended-Tofts Model. ISMRM. 2016. p.0868.
5. Velikina J V, Alexander AL, Samsonov A. Accelerating MR parameter mapping using sparsity-promoting regularization in parametric dimension. MRM. 2013 Nov; 70(5):1263–73.
6. Barnes SR, Ng TSC, Santa-Maria N, Montagne A, Zlokovic B V., Jacobs RE. ROCKETSHIP: a flexible and modular software tool for the planning, processing and analysis of dynamic MRI studies. BMC Med Imaging. BMC Medical Imaging; 2015;15(1):19.
7. Guo Y, Lebel RM, Zhu Y, Lingala SG, Shiroishi MS, Law M, Nayak K. High-resolution whole-brain DCE-MRI using constrained reconstruction: prospective clinical evaluation in brain tumor patients. Med Phys 2016;43:2013–2023.
8. Zhu Y, Guo Y, Lingala SG, Marc Lebel R, Law M, Nayak KS. GOCART: GOlden-angle CArtesian randomized time-resolved 3D MRI. Magn Reson Imaging 2016;34:940–950.
9. Tae Jin Yun, Chul-Kee Park, Tae Min Kim, et al. Glioblastoma Treated with Concurrent Radiation Therapy and Temozolomide Chemotherapy: Differentiation of True Progression from Pseudoprogression with Quantitative. Radiology. 2015;274:830–40.
Figures