1194
Gaussian and non-Gaussian diffusion models for Differential Diagnosis of Prostate Cancer with in bore Transrectal MR-Guided Biopsy as a Pathological Reference1Beijing Hospital, Beijing, People's Republic of China, 2GE Healthcare, China
Synopsis
This study is to compare the utility of various metrics derived from different models based DWI and DKI in the differential diagnosis of prostate cancer. ADC, ADCslow, DDC, and MD values were significantly lower while MK value was significantly higher in prostate cancer lesions than those of prostatitis and BPH. Parameters derived from both Gaussian and non-Gaussian models could characterize prostate cancer. Diagnosis performance benefit was observed for DKI model as compared to MEM.
Purpose
Diffusion-weighted imaging (DWI) has been usedextensively for the diagnosis of prostate cancer, it is generally accepted that ADC values are lower in prostate cancer than those of noncancerous tissues [1]. However, ADC values of prostate cancer may overlap substantially with those of noncancerous tissues, such as prostatitis and benign prostatic hyperplasia (BPH). This could be potentially due to the underlying Gaussian diffusion model, which derives from the actual diffusion process. Several studies have evaluated the utilities of non-Gaussian diffusion models including intra-voxel inherent motion (IVIM) [2], stretched exponential model (SEM) [3] or diffusion kurtosis imaging (DKI) [4] in the diagnosis of prostate cancer, however contradicting results were reported. A potential drawback of the past studies is that pathological confirmations were performed using transrectal ultrasound (TRUS)-guided biopsy, which features limited accuracy of only up to 40%. In addition, past studies mainly focused on the identification of the cancer, whereas differentiation of cancer and noncancerous tissues has been rarely attended. In this work, a thorough comparison of the differential diagnosis ability of Gaussian and non-Gaussian (IVIM, SEM and DKI) models was performed using in bore MR guided biopsy as a reference, which features much improved accuracy compared to TRUS-guided biopsy.Methods
This retrospective study was approved by the local institutional review board. A total of 80 patients with suspected prostate cancer as indicated by elevated prostate specific antigen (PSA) (>4 ng/mL) and/or palpable prostatic nodule, without any prior treatment, were enrolled and underwent MR examination. Single b value, multi-b value, multi-b multi-direction diffusion imaging (Table 1) were performed on a 3.0T whole body scanner (Discovery MR750, GE, WI) with an 8-channel cardiac coil. Targeted biopsy of suspicious lesions were performed under the guidance of both T2 and on DWI images. In total, 62 lesions were obtained (2 each for 22 patients and 3 each for 6 patients), including 24 prostate cancers, 21 prostatitis and 17 benign prostatic hyperplasia (BPH). Independent t-test was used to test the differentiating ability of various derived metrics between prostate cancer and noncancerous lesions (bothprostatitis and BPH). Receiver operating characteristic (ROC) curves were also obtained and compared among different metric to investigate which metric features superior detection accuracy.Results
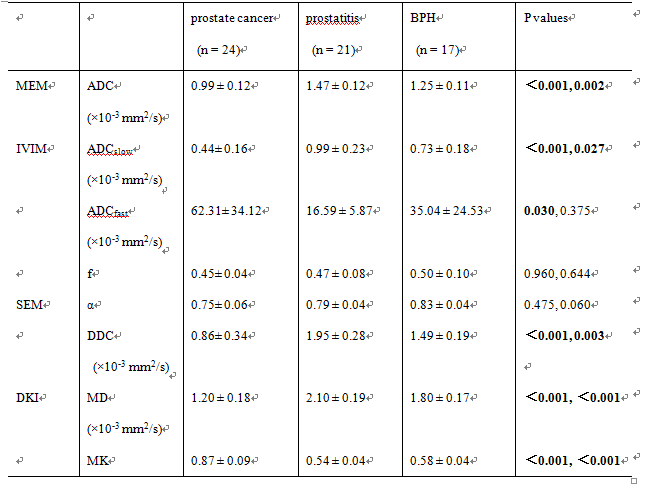
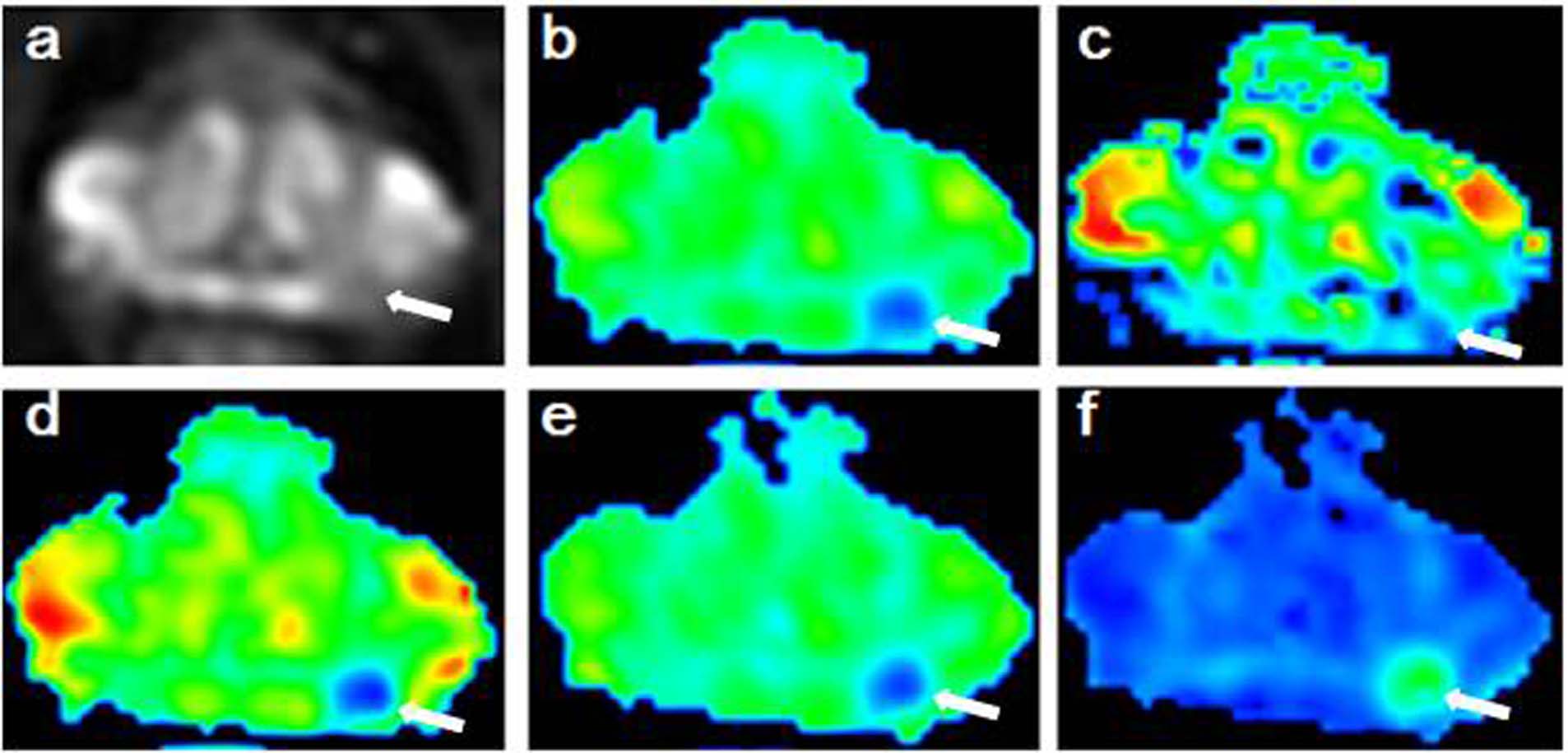
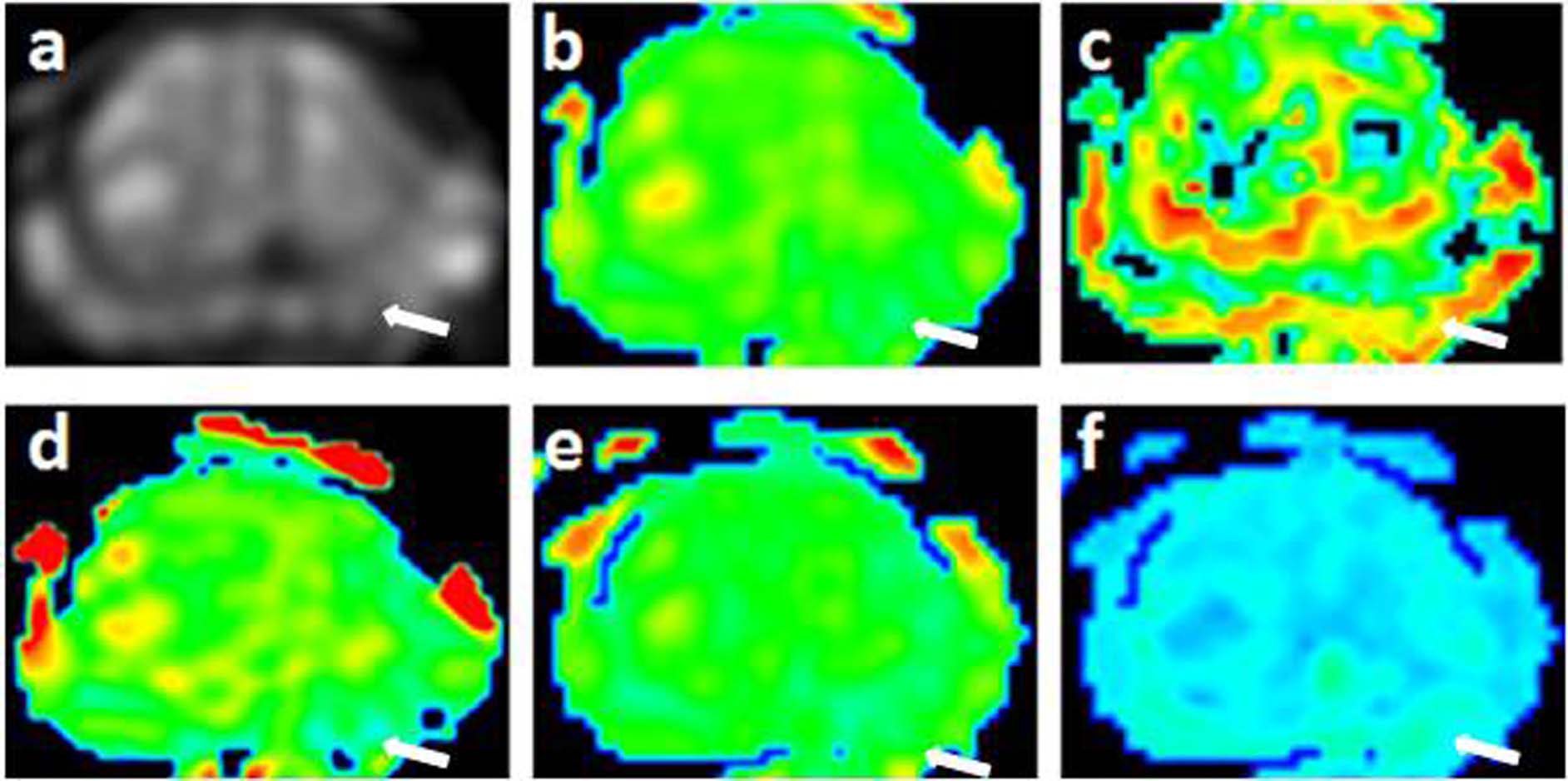
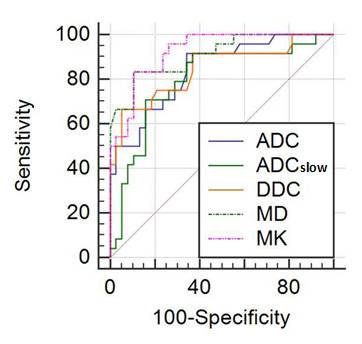
The ROI based measurements of various parameters are shown as mean±95% CI in Table 2, along with the p values corresponding to the correlation between prostate cancer and prostatitis and BPH. It can be seen that ADC, ADCslow, DDC and MD values were lower in prostate cancer than in prostatitis or BPH with statistical significance; MK value was higher in prostate cancer lesions than in prostatitis or BPH with statistical significance; ADCfast was higher in prostate cancer lesions than in prostatitis with statistical significance but no statistical significance was observed between prostate cancer and BPH; α and f values showed no statistical significances between prostate cancer and noncancerous tissues. A case with prostate cancer and acase with prostatitis were shown in Figs 1 and 2 respectively. The area under curve (AUC) of ADC, ADCslow, DDC, MD and MK are 0.841, 0.796, 0.845, 0.909, and 0.925 respectively. The AUC of MK showed higher value than that of both ADC and ADCslow, with statistical significance. The AUC of MD showed higher value than that of ADCslow, with statistical significance. No statistically significant differences were observed between other parameters.Discussion and conclusion
This study compared the use of various parametric metrics derived from Gaussian and different non-Gaussian diffusion models in the differential diagnosis of prostate cancer from noncancerous lesions. In bore MR guided biopsy was as pathological reference for improved accuracy. It was seen that the parameter MK showed the highest AUC, and the statistical difference was observed between MK and ADC, as well as MK and ADCslow. Hence it may be concluded that the differential diagnosis ability of MK is superior to that of conventional ADC. Based on the results, it may be concluded parameters derived from both Gaussian and non-Gaussian models may differentiate prostate cancer from prostatitis and BPH. Diagnosis performance benefit was observed for DKI model as compared to MEM.Acknowledgements
This work was supported by grants from Beijing Hospital Nova Project.References
[1] Kobayashi H, Kitamura K, Mizukami S, Hanazawa K, Sakamoto Y (2013) Diffusion-weighted imaging for prostate cancer localization: comparison of apparent diffusion coefficient values in cancerous and non-cancerous tissues, and the Gleason score of the radical prostatectomy specimens. Nihon Hinyokika Gakkai zasshi 104: 489-495
[2] Kuru TH, Roethke MC, Stieltjes B, et al (2014) Intravoxel incoherent motion (IVIM) diffusion imaging in prostate cancer - what does it add? J Comput Assist Tomogr 38:558-564
[3] Liu X, Zhou L, Peng W, Wang H, Zhang Y (2015) Comparison of stretched-Exponential and monoexponential model diffusion-Weighted imaging in prostate cancer and normal tissues. J Magn Reson Imaging 42:1078-1085
[4] Suo S, Chen X, Wu L, et al (2014) Non-Gaussian water diffusion kurtosis imaging of prostate cancer. Magn Reson Imaging 32:421-427
Figures