1134
Preoperative assessment of tumor stiffness and tumor-brain adhesion in patients with vestibular schwannoma using MR elastography-based method1Department of Radiology, Ohio State University Wexner Medical Center, Columbus, OH, United States, 2Department of Otolaryngology, Ohio State University Wexner Medical Center, Columbus, OH, United States, 3Department of Neurological Surgery, Ohio State University Wexner Medical Center, Columbus, OH, United States
Synopsis
Microsurgery in vestibular schwannoma patients aims to complete tumor resection without compromising any neurological functionality. Inadequate preoperative knowledge of tumor may prolong surgical time and increase risk of postoperative complications. Previous studies have used magnetic resonance elastography (MRE) based method to determine tumor stiffness and tumor-brain adhesion, separately. But none of the studies have investigated tumor stiffness and tumor-brain adhesion together. The aim of this study is to bring together the two MRE-based outcomes – tumor stiffness and tumor-brain adhesion – and correlate with surgical findings. Preliminary results show a good correlation between preoperative assessment of tumor and surgical findings.
Purpose
For decades, patients with vestibular schwannoma (VS) have been treated with microsurgery that aims to complete tumor resection while preserving facial and hearing nerves1,2. Surgery involves peeling tumor off the brain as well as resecting, which depends upon tumor-brain adhesion and tumor stiffness, respectively. Inadequate preoperative knowledge of tumor like tumor stiffness and tumor-brain adhesion may prolong surgical time and increase risk of postoperative complications3. One study has shown stiffness estimates using magnetic resonance elastography (MRE) in patients with brain tumors including VS and found a significant correlation with tumor consistency during surgery4. Another study has investigated tumor-brain adhesion in VS patients by processing MRE wave data with two different algorithms, octahedral shear strain (OSS) as well as shear line analysis, and have shown good correlation with surgical findings5. As per our knowledge, none of the earlier studies have investigated both the tumor stiffness and tumor-brain adhesion together. The aim of this study is to bring together the two MRE-based outcomes – tumor stiffness and tumor-brain adhesion – and correlate with the clinical assessment done by surgeons during surgery.Methods
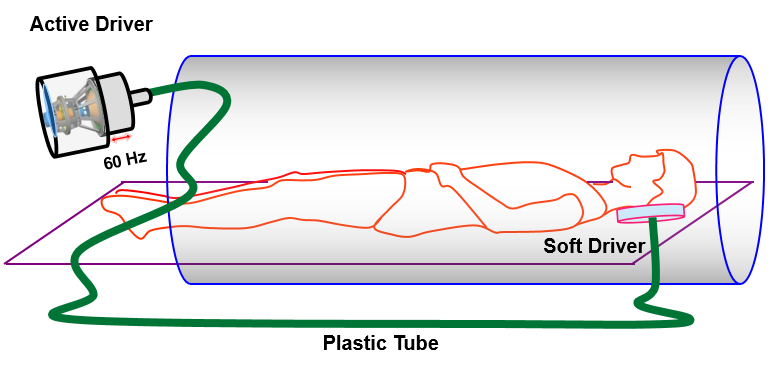
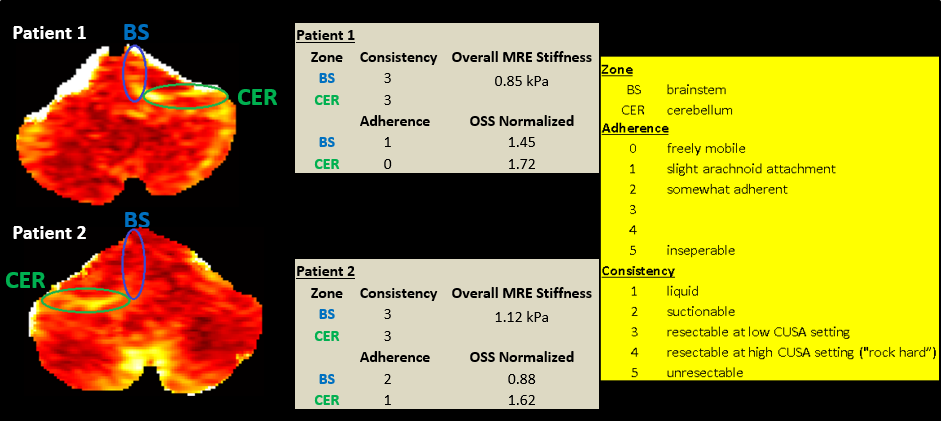
All imaging was performed using a 3T MRI scanner (Tim Trio, Siemens Healthcare, Erlangen, Germany). Written informed consent was obtained from all patients (n=4). Axial slices were obtained using a gradient echo (GRE) MRE sequence. T2-weighted fluid-attenuated inversion recovery (FLAIR) image was acquired to clearly identify the tumor-brain interface. Experimental set up is shown in figure 1. 60 Hz vibrations were introduced through a soft pillow-like driver that sits underneath head in brain coil. Imaging parameters included: FOV=256x256 mm2, matrix size=256x256, slice thickness=3 mm, number of slices vary as per tumor size, MRE phase offsets=4. Motion encoding gradient of 60 Hz was applied separately in the x, y and z directions to encode in-plane and through plane displacement fields. Scan time was 15-20 minutes depending on number of slices acquired. MRE images were masked to obtain the brain and a curl processing was performed to remove longitudinal component of motion. Additionally, directional filter was applied to remove the reflected waves. Finally, 3D local frequency estimation was performed to obtain weighted stiffness map using MRE-Lab (Mayo Clinic, Rochester, MN). ROI was drawn slightly away from brain boundary to avoid any edge effects. On MRE data, OSS6 algorithm was applied to determine shear strain measurements at the tumor-brain interface to quantify the degree of adhesion. OSS map from each patient was then normalized using median since the vibrations reaching the tumor-brain interface may vary in amplitude from patient to patient depending on anatomy, tumor location and contact with soft driver. Mean value from ten randomly selected pixels on tumor-brain interface from brainstem (BS) and cerebellum (CER) regions is reported for OSS. Blinded to the preoperative results, neurosurgeons qualitatively assessed tumor consistency (scale 1 to 5) and adherence (scale 0 to 5) for BS and CER regions during surgery as shown in figure 3. Thus far, qualitative assessment by surgeons is only performed in two out of four patients and is reported in this study.Results
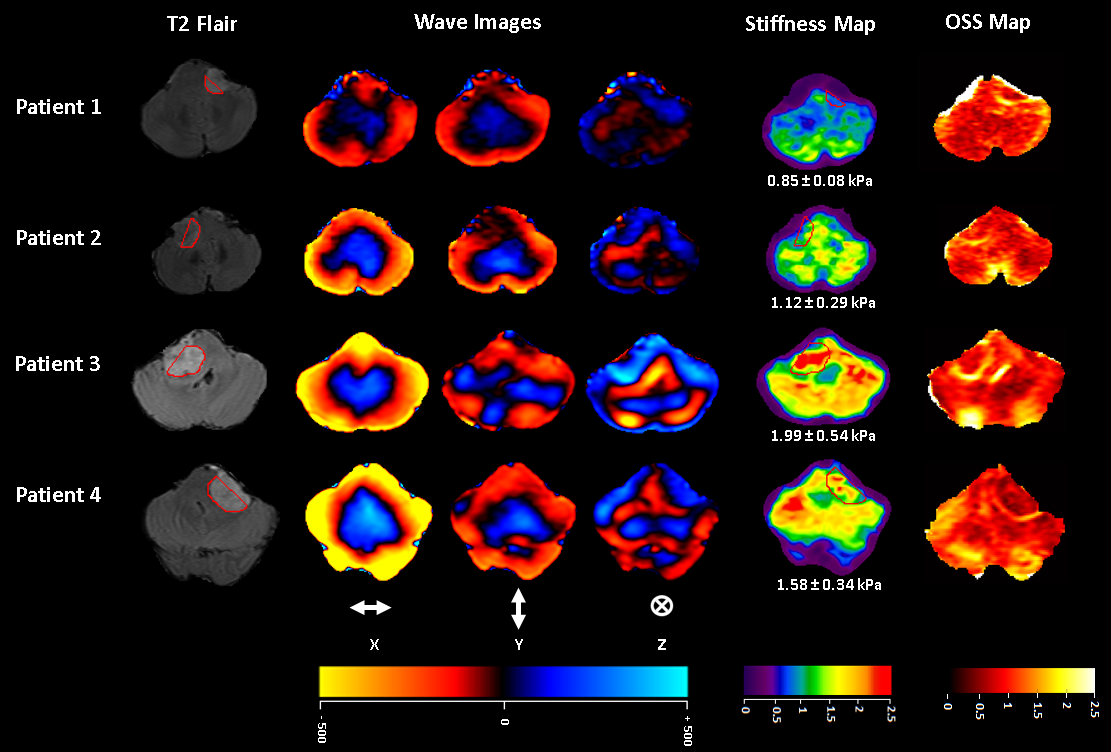
Figure 2 displays a short-axis slice from four patients showing T2-weighted FLAIR image used to identify tumor boundary, snapshot of one of the time points of wave propagation in three spatial directions, the corresponding 3D stiffness and normalized OSS map. Figure 3 shows qualitative assessment scores by surgeons for tumor consistency and adherence and compare it with preoperative MRE stiffness and normalized OSS value at BS and CER regions. In patient 1, high shear strain value from normalized OSS map i.e. 1.72 in CER region correlate to score 0 i.e. freely mobile given by surgeons. Similarly, low OSS value of BS region in patient 2 i.e. 0.88 correlate to score 2 i.e. somewhat adherent. For patient 1 and 2, mean stiffness from one slice was found to be 0.85±0.08 kPa and 1.12±0.29 kPa, respectively which correlate to score 3 for consistency i.e. resectable at low CUSA setting.Discussion
Although the sample size is small (n = 4), preliminary results demonstrate that MRE based stiffness estimates and normalized OSS measurements correlate well with the tumor consistency and adherence assessed by surgeons during surgery in VS patients. Currently, we are expanding the dataset to get a big sample size.Conclusion
MRE-based method can potentially be used preoperatively to assess the tumor stiffness and tumor-brain adhesion, which can predict surgical time and postoperative complications in patients with VS.Acknowledgements
Funded by NIH R01HL124096 and AHA 13SDG14690027References
1. Sampath, P., Holliday, M. J., Brem, H., et al. Facial nerve injury in acoustic neuroma (vestibular schwannoma) surgery: etiology and prevention. Journal of neurosurgery, 1997; 87(1), 60-66.
2. Brackmann, Derald E., Robert M. Owens, Rick A. Friedman, et al. Prognostic factors for hearing preservation in vestibular schwannoma surgery. Otology & Neurotology 21, no. 3 (2000): 417-424.
3. Darrouzet, V., Martel, J., Enée, V., et al. Vestibular schwannoma surgery outcomes: our multidisciplinary experience in 400 cases over 17 years. The Laryngoscope, 2004; 114(4), 681-688.
4. Sakai, N., Takehara, Y., Yamashita, S., et al. Shear Stiffness of 4 Common Intracranial Tumors Measured Using MR Elastography: Comparison with Intraoperative Consistency Grading. American Journal of Neuroradiology, 2016; 37(10), pp.1851-1859.
5. Yin, Z., Glaser, K. J., Manduca, A., et al. Slip interface imaging predicts tumor-brain adhesion in vestibular schwannomas. Radiology, 2015; 277(2), 507-517.
6. McGarry, M. D. J., Van Houten, E. E. W., Perrinez, P. R., et al. An octahedral shear strain-based measure of SNR for 3D MR elastography. Physics in medicine and biology, 2011; 56(13), N153.
Figures