1025
Highly efficient respiratory motion corrected dual-phase coronary MR angiography in a 3T PET-MR system1Division of Imaging Sciences and Biomedical Engineering, King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare, Frimley, United Kingdom
Synopsis
Respiratory motion remains a major challenge for dual-phase coronary MR angiography (CMRA). Here we propose an efficient acquisition and reconstruction scheme, that allows for inline 2D translational and offline 3D non-rigid motion-corrected systolic and diastolic CMRA using image-based navigators. Results from healthy volunteers show that motion correction improves visualization of the right and left coronary arteries in both cardiac phases. The proposed scheme potentially allows for comprehensive diagnosis of coronary artery disease using simultaneous PET-MR by acquiring coronary anatomy and left-ventricular function with the dual-phase CMRA and myocardial perfusion/viability with PET in an efficient cardiac and respiratory motion-compensated framework.
Introduction
Dual-phase coronary MR angiography (CMRA) allows for simultaneous visualization of the coronary lumen integrity and assessment of cardiac function, being a promising tool for the comprehensive diagnosis of coronary artery disease(1). Recently, new approaches have been proposed to improve efficiency of dual-phase CMRA at 1.5T, using image-based navigators (iNAVs) to address the problem of respiratory motion(2). Here we propose to extend this approach to a 3T system, using a gradient echo sequence with a golden-step Cartesian spiral (G-CASPR(3)) trajectory, jointly with a motion-corrected reconstruction framework(4) to account for the complex non-rigid respiratory motion of the heart directly in the reconstruction. Low-resolution coronal-oriented 2D iNAVs are independently acquired for systole and diastole to estimate foot-head and right-left translational motion in a beat-to-beat fashion, so that inline 2D translational and offline 3D non-rigid motion-corrected dual-phase CMRA imaging can be performed. The proposed approach also provides non-rigid respiratory motion fields and non-rigid cardiac motion fields (between systole and diastole) that can be used to correct for simultaneously acquired PET data in a 3T PET-MR system.Methods
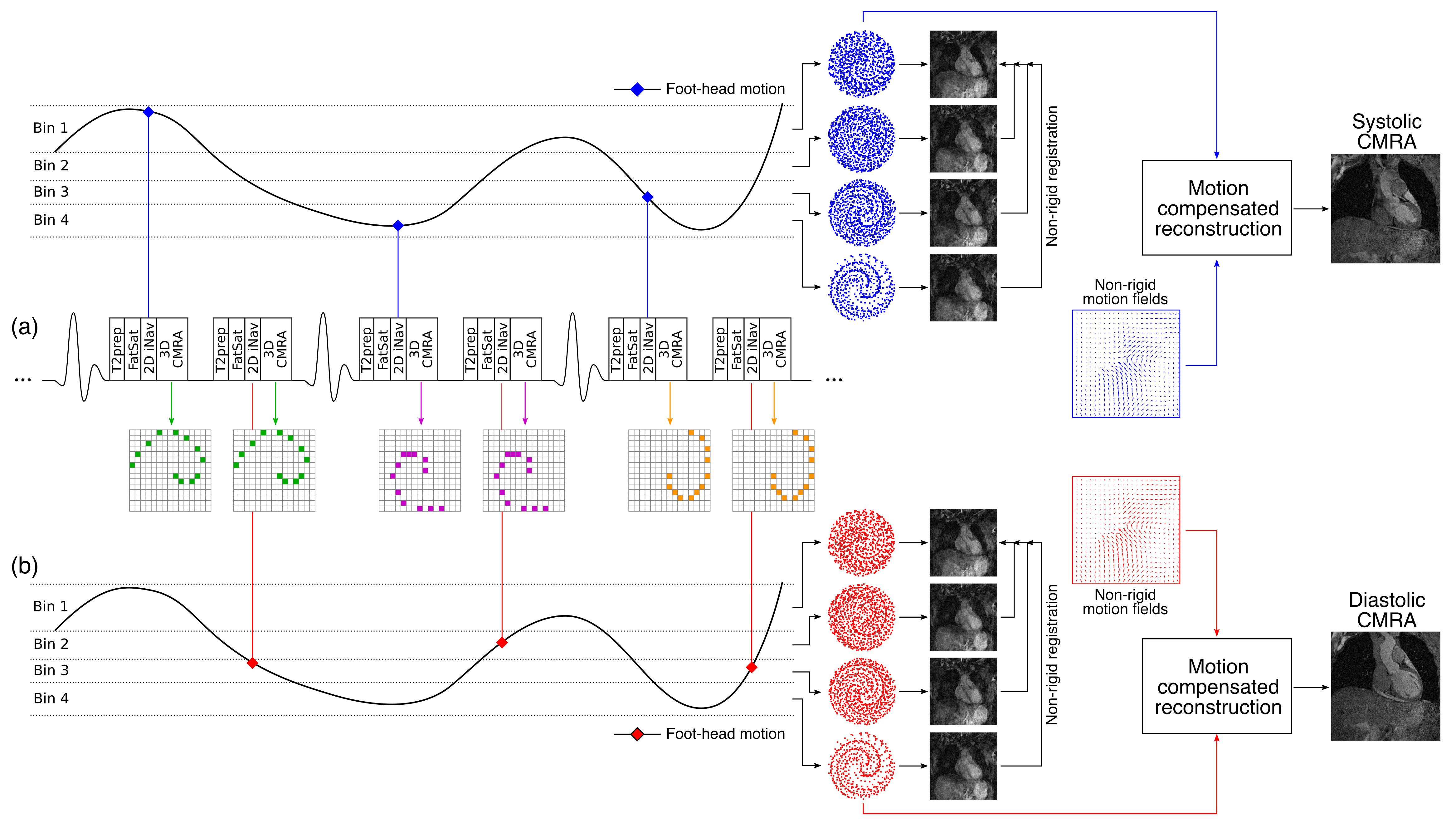
The proposed dual-phase CMRA acquisition and reconstruction scheme is shown in Fig1. An ECG-triggered 3D T1-weighted spoiled gradient echo sequence with a fully sampled G-CASPR trajectory was implemented so that each spiral interleaf is acquired both in systole and diastole (Fig1a). An adiabatic T2 preparation pulse (T2prep) and a fat saturation (FatSat) prepulse are applied before 3D CMRA acquisition to enhance the contrast between the coronary arteries and surrounding tissues without the use of contrast agents. Foot-head motion estimated from each set of iNAVs is used to bin the CMRA data acquired at the corresponding cardiac phase (Fig1b). For each cardiac phase, binned CMRA data reconstructed at each respiratory position is used to estimate 3D non-rigid motion fields in a bin-to-bin fashion. The motion fields are then directly included in the reconstruction of the CMRA data(4), so that one non-rigid respiratory motion-corrected CMRA image is reconstructed per cardiac phase.
Results
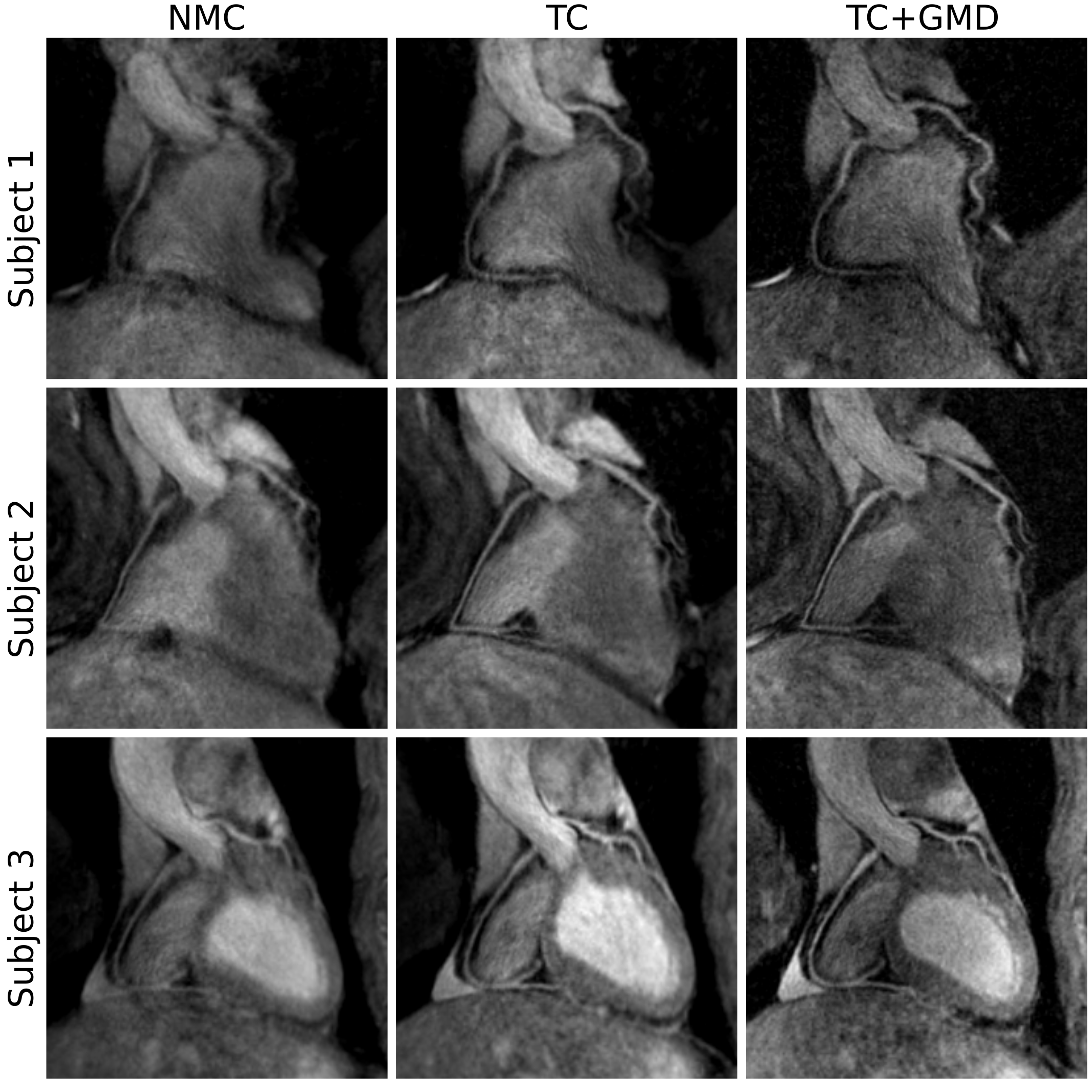
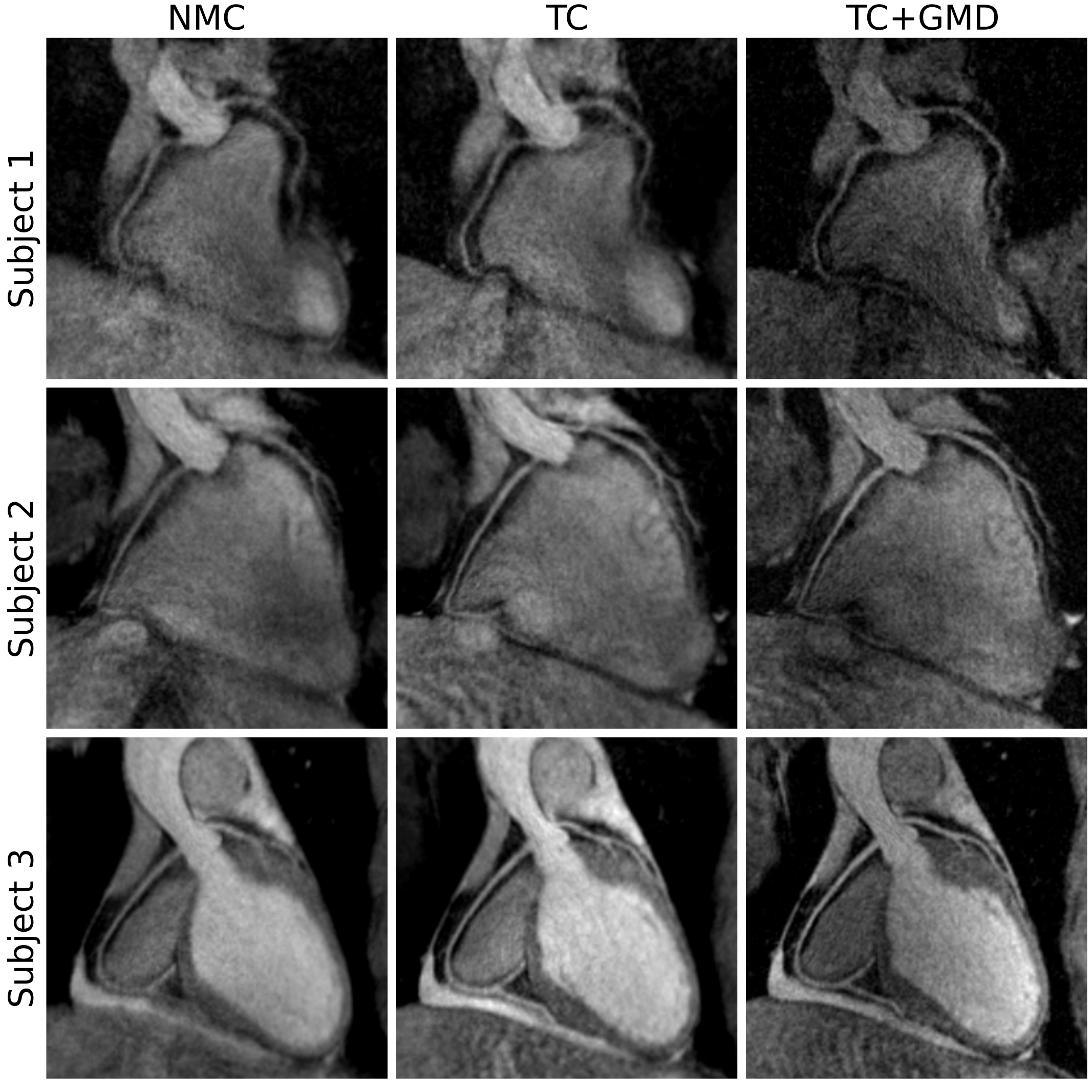
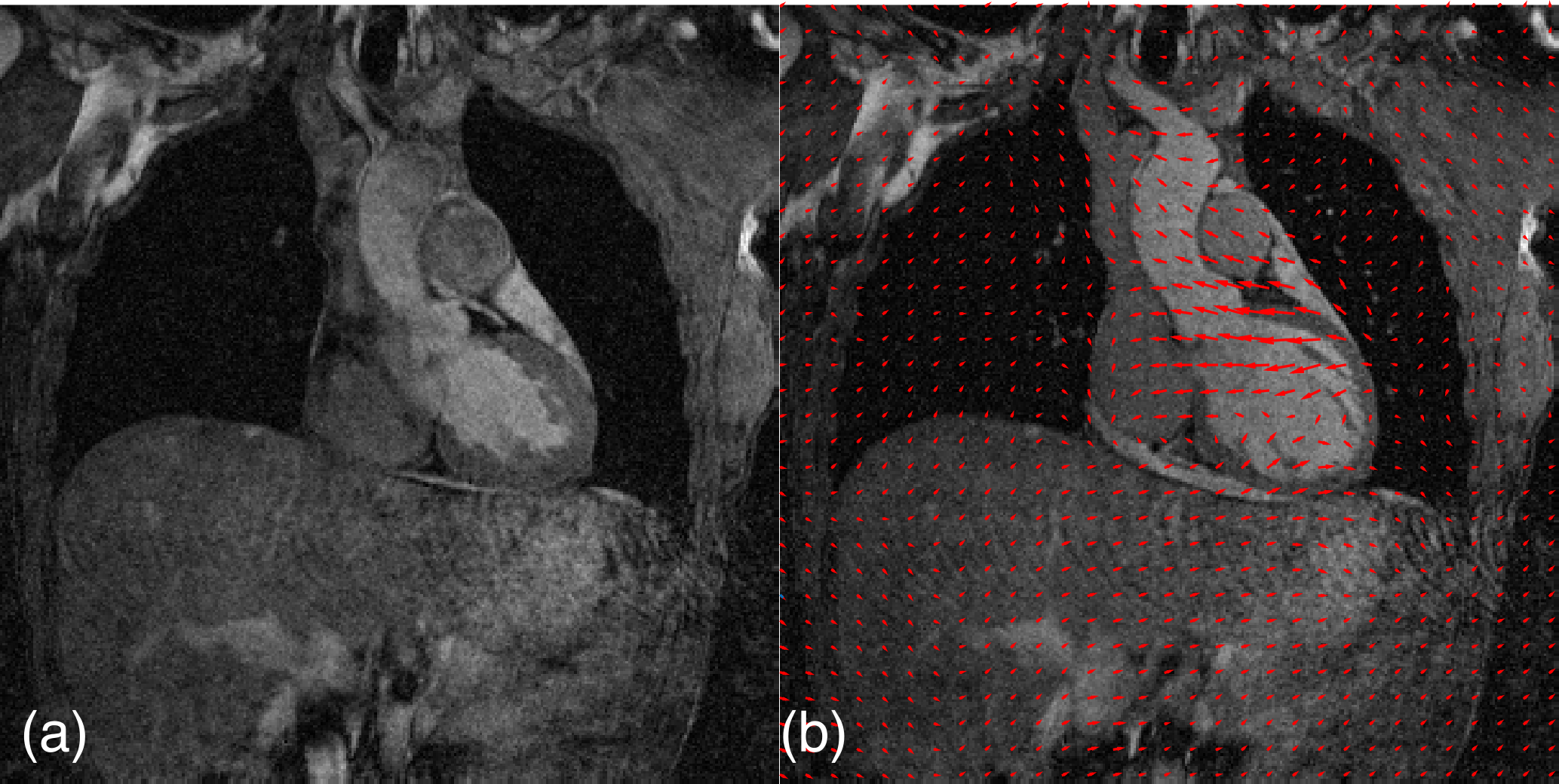
Systolic and diastolic 3D CMRA images were reformatted to simultaneously visualize the left anterior descending (LAD) and right coronary artery (RCA). Significant improvements in visualisation of the distal RCA can be observed for systolic images when applying TC for all the subjects (Fig2). TC+GMD images show further improvement in image quality, increasing the visible length and sharpness of the vessels. A similar behaviour was observed when analysing diastolic images (Fig3). Improvements in the visualisation of the RCA and LAD are apparent when applying TC+GMD, showing a better depiction of the distal segment of the vessels. Fig4 shows an example motion corrected coronal slice in systole and diastole, with overlaid non-rigid motion fields that represent the deformation of the heart from diastole to systole.
Three healthy subjects were scanned on a Biograph mMR scanner (Siemens Healthcare, Germany) using a prototype implementation of the proposed dual-phase CMRA sequence (304x304x40-48 matrix size, 1x1x2mm3 resolution, TR/TE=3.7/1.7ms, FA=12°, T2prep=50ms). Two subject-specific trigger delays were set targeting the mid-systolic and mid-diastolic rest period and an acquisition window ranging from 89 to 111ms was used. For each iNAV, 14 start-up echoes (same FOV, FA=3º) were used. Each dataset was reconstructed (a) with no motion correction (NMC), (b) with foot-head and right-left translational correction only (TC) and (c) with translational plus non-rigid motion correction (TC+GMD).
Conclusion
We have presented an MR acquisition scheme that allows for inline 2D translational and offline 3D non-rigid motion-corrected dual-phase coronary MR angiography in a 3T PET-MR scanner. Motion estimated in a beat-to-beat and bin-to-bin fashion was used to correct the CMRA data producing high-resolution images that allow for visualisation of the coronary arteries. The proposed motion correction scheme improves image quality and contrast compared with uncorrected images for both systole and diastole. Further work includes assessing cardiac function indices (i.e. ejection fraction) and estimating cardiac motion from the reconstructed dual-phase CMRA images, so that respiratory and cardiac motion estimates can be used for correcting simultaneously acquired cardiac viability PET data.Acknowledgements
The authors acknowledge financial support from: (1) EPSRC: EP/N009258/1, (2) King’s College London & Imperial College London EPSRC Centre for Doctoral Training in Medical Imaging (EP/L015226/1).References
(1) Gotschy A et al. Cardiovascular magnetic resonance for the assessment of coronary artery disease. Int J Cardiol 2015;193:84–92
(2) Henningsson M et al. Dual-phase coronary MR angiography using image based respiratory navigation. In: Proceedings ISMRM 2016
(3) Prieto C et al. Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. J Magn Reson Imaging 2015;41:738–746
(4) Cruz G et al. Highly efficient nonrigid motion-corrected 3D whole-heart coronary vessel wall imaging. Magn Reson Med 2016. doi: 10.1002/mrm.26274.2
Figures