1023
Evaluation of Self-Navigated Golden-Angle Ordered Conical Ultrashort Echo Time (UTE) MRI of the Abdomen on Pediatric Patients in Multiple Sedation States1Radiology, Stanford University, Stanford, CA, United States, 2Applied Science Laboratory, GE Healthcare, San Diego, CA, United States
Synopsis
To assess the feasibility of conical k-space trajectory free-breathing UTE abdominal MRI and the effects on image quality of 50% data subsampling (thereby potentially shortening scans) and soft-gated motion correction reconstruction techniques, 42 consecutive pediatric patients were recruited and scanned. The images were scored in blinded fashion by two readers. Adequate delineation was obtained for all evaluated abdominal structures except the hepatic artery. 50% subsampling decreased image quality only slightly, favoring the implementation of a shorter scan time with negligible diagnostic compromise. Overall, motion correction mildly degraded image quality, possibly due to greater noise from data subsampling.
PURPOSE
Three-dimensional (3D) radial UTE magnetic resonance (MR) imaging has been evaluated for a variety of clinical scenarios, including musculoskeletal and pulmonary applications1,2,3. 3D UTE imaging utilizing conical k-space sampling permits greater scan efficiency than radial acquisitions, while still diffusing motion and aliasing artifacts, rendering images relatively robust to flow and motion. Given the motion of upper abdominal organs during the respiratory cycle, these characteristics may make conical-trajectory UTE imaging a suitable free-breathing technique. Here we aim to develop a golden-angle ordered conical UTE MR technique to further diffuse motion artifacts, assess the utility of 50% data subsampling to decrease scan time, and use central k-space data phase for self-navigation and associated soft-gated motion correction. We assess the clinical performance of the technique for pediatric patients undergoing 3T MRI.METHODS
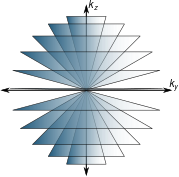
Data were acquired using an RF-spoiled GRE sequence with a three-dimensional conical k-space sampling trajectory4,5 (Figure 1). The acquisition of each interleaf was ordered according to the golden-ratio permutation to increase motion robustness and to enable retrospective data subsampling. The DC signal from each conical interleaf was processed to compute motion waveforms. Images were reconstructed using either gridding, soft-gated parallel imaging and compressed sensing (PI & CS)6,7, or PI & CS with no soft-gating. All reconstructions were performed using the Berkeley Advanced Reconstruction Toolbox8. With IRB approval, 42 consecutive pediatric patients referred for abdominal MRI at 3T were retrospectively identified (mean age: 8.5 years, range: 5.5 months-22.0 years; 28 male), most (38, 90.5%) with gadobutrol, and half without anesthesia.
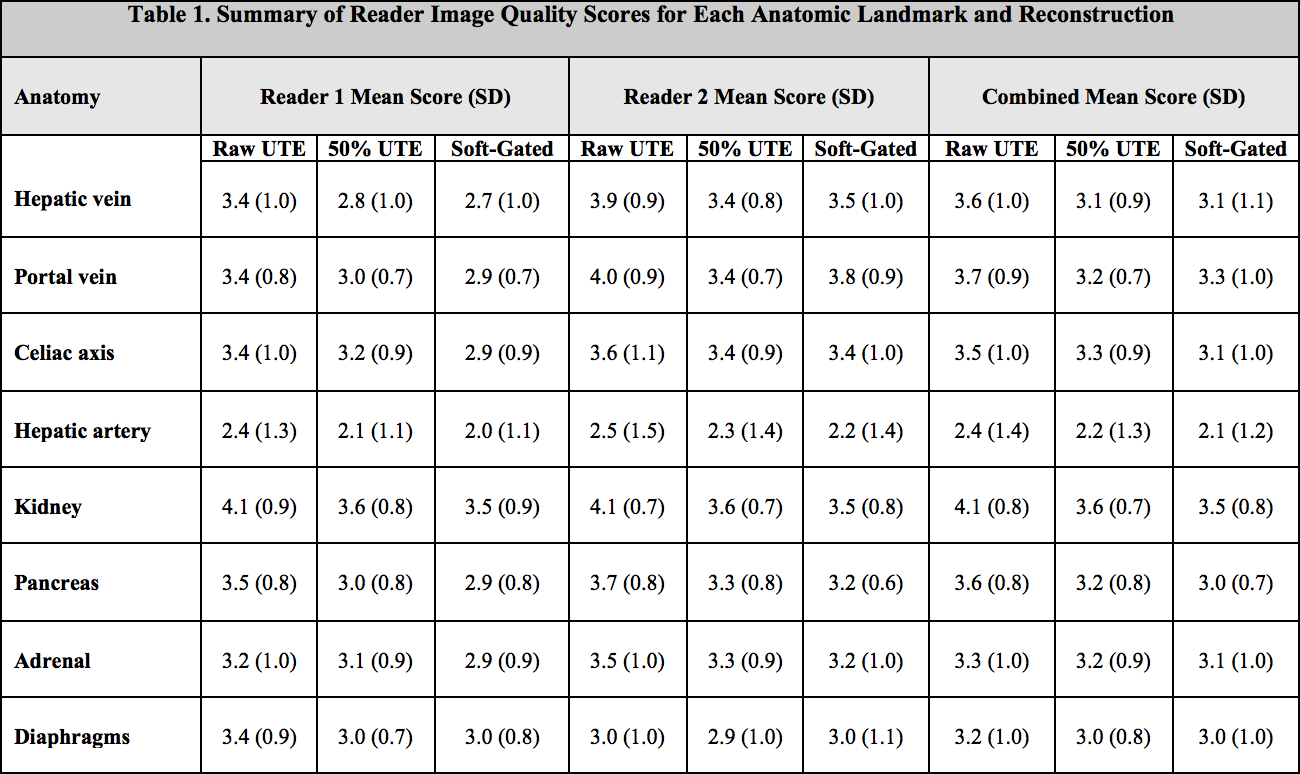
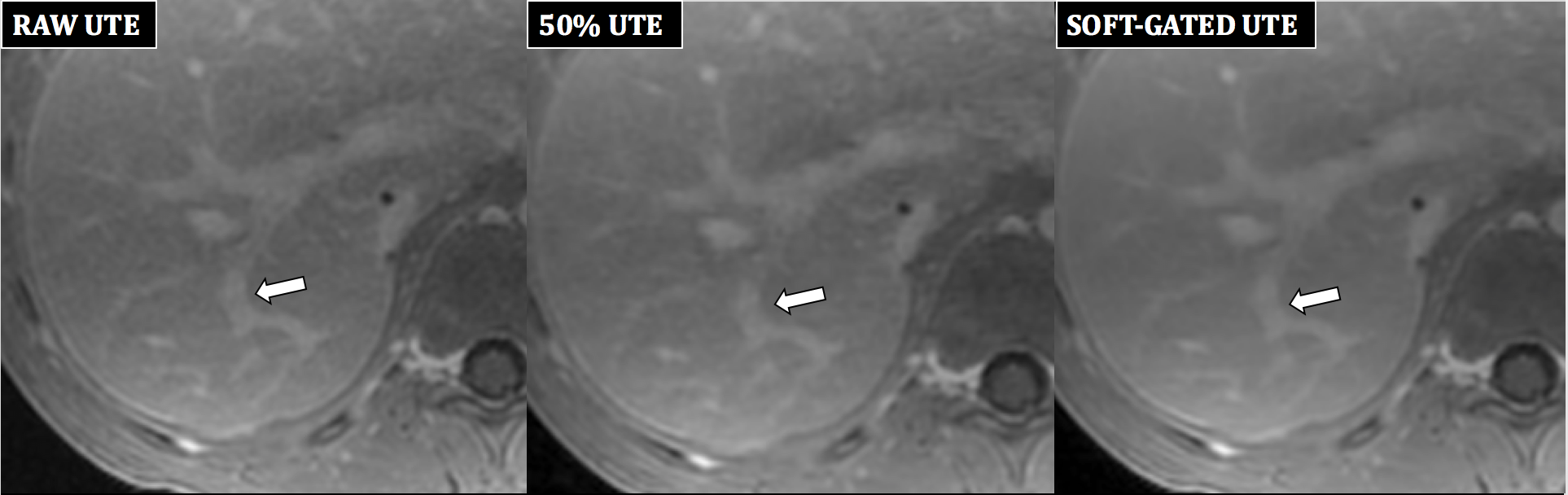
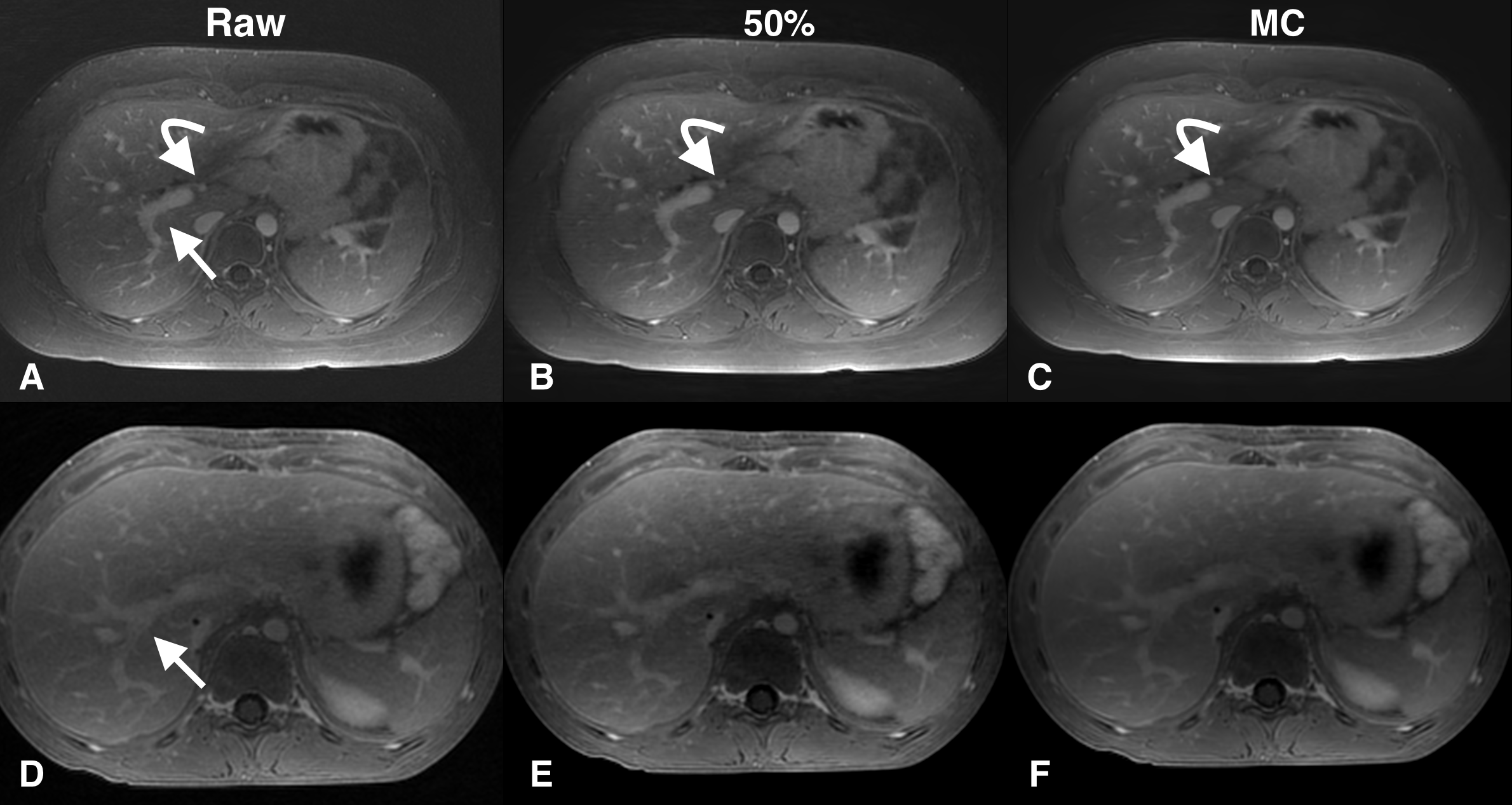
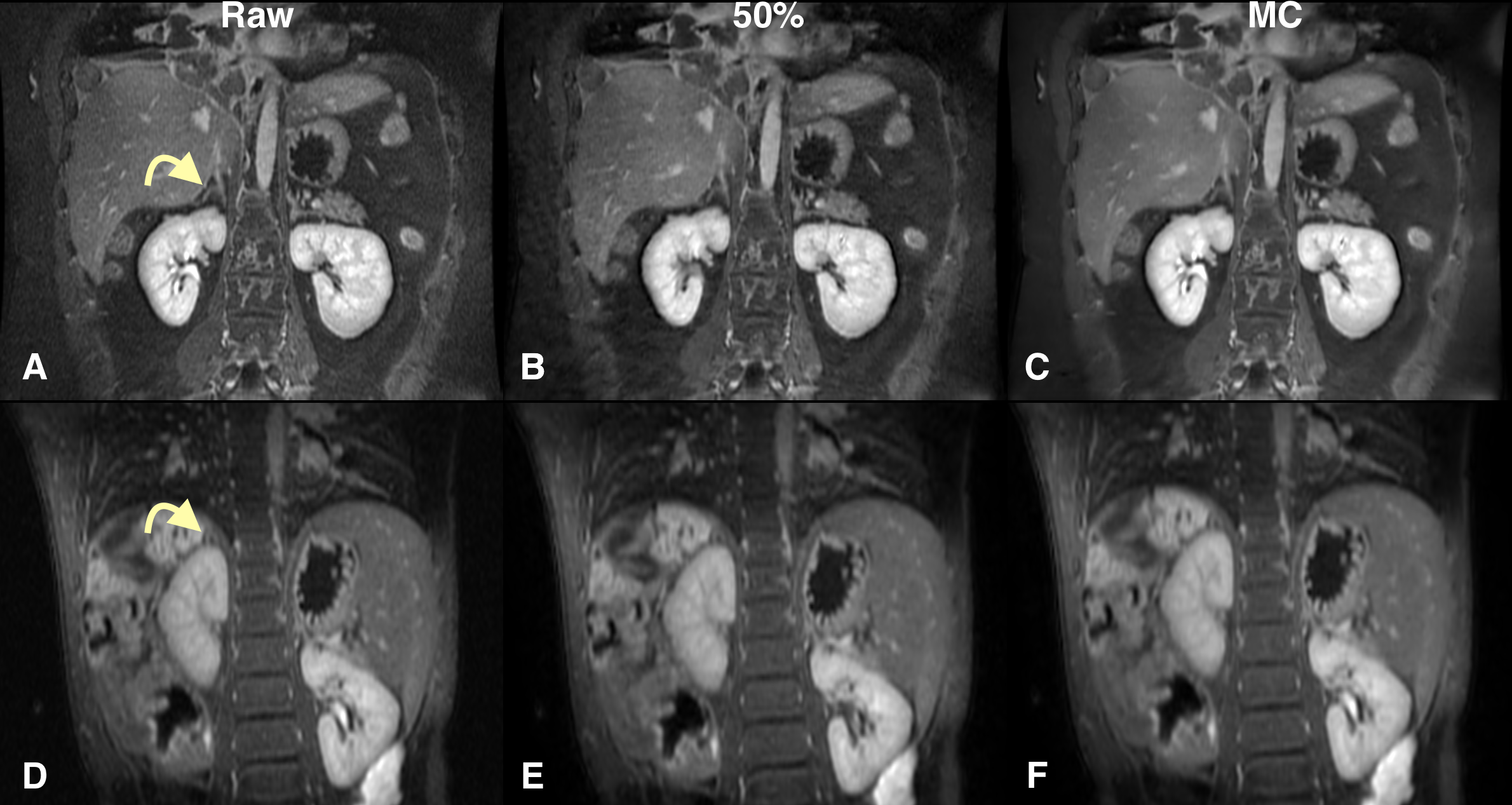
From UTE k-space data, three image sets were reconstructed and submitted for evaluation: (i) one with all data, (ii) one using the first 50% of data, and (iii) a final set with soft-gating motion correction that effectively utilizes the expiratory half of data. Using a five-point Likert scale (1=non-diagnostic, 2=limited, 3=adequate, 4=good, 5=excellent), two blinded radiologists independently scored image quality of the right hepatic vein (RHV), right portal vein (RPV), celiac axis, common hepatic artery (CHA), right kidney (RK), pancreas, right adrenal (RA), and thoracic diaphragm. The null hypothesis of no significant difference in scores was assessed using a Wilcoxon signed rank test. Interobserver agreement was assessed with the intra-class correlation coefficient (ICC).
RESULTS
For full data (raw) UTE, combined mean scores for all landmarks except CHA were >=3, ranging from 3.2 ± 1.0 for diaphragm to 4.1 ± 0.8 for RK. Table 1 shows a summary of scores. Interobserver agreement was good to excellent for combined scores (ICC=0.74). Compared to full data UTE, 50% subsampling degraded quality for all landmarks (P<0.02 for all structures), but the mean score decrease ranged from 0.1-0.5. Motion correction also degraded image quality for all landmarks (P<0.002 for all structures, except diaphragm: P=0.08). However, in select cases, reader 2 scored the RHV or RPV better with soft-gating compared to raw UTE (Figure 3). In a subanalysis of 14 intubated patients, motion correction again degraded image quality for all landmarks including the diaphragm (P=0.0093), but in the 21 nonsedated patients, there was no significant difference of mean scores for multiple landmarks. Notably, diaphragm scores in the nonsedated patients were not significantly different between full data UTE and motion corrected images (2.8 ± 0.9 vs. 2.9 ± 0.9, p=0.3614).DISCUSSION
Diagnostic delineation of abdominal anatomy can be obtained with a free-breathing UTE sequence, though the hepatic artery was often not well seen, likely due to its small size and the delayed phase non-MRA technique. Reducing scan time (to 150 seconds) is unlikely to compromise image quality. The motion robustness of the acquisition was observed, and soft-gated motion correction is unlikely to improve image quality, possibly due to greater noise from effective data subsampling. In cases with greater motion (nonsedated patients), it may improve quality.CONCLUSION
Free-breathing conical k-space trajectory UTE abdominal MRI is feasible, with diagnostic image quality. Overall, motion correction slightly degraded images, possibly due to greater noise from data subsampling. However, in select nonsedated cases, motion-correction may improve delineation of some structures.Acknowledgements
Research support from GE Healthcare, and support of NIH R01EB009690.References
1. Herrmann K-H, Krämer M, Reichenbach JR (2016) Time Efficient 3D Radial UTE Sampling with Fully Automatic Delay Compensation on a Clinical 3T MR Scanner. PLoS ONE 11(3): e0150371. doi:10.1371/journal.pone.0150371
2. Johnson KM, Fain SB, Schiebler ML, Nagle S. Optimized 3D ultrashort echo time pulmonary MRI. Magn Reson Med 2012 Dec 4.
3. Tibiletti, M., Bianchi, A., Kjørstad, Å., Wundrak, S., Stiller, D. and Rasche, V. (2016), Respiratory self-gated 3D UTE for lung imaging in small animal MRI. Magn. Reson. Med. doi:10.1002/mrm.26463
4. Carl, M., Bydder, G. M. & Du, J. UTE imaging with simultaneous water and fat signal suppression using a time-efficient multispoke inversion recovery pulse sequence. Magn Reson Med 0, 1–6 (2015).
5. Gurney, P. T., Hargreaves, B. A. & Nishimura, D. G. Design and analysis of a practical 3D cones trajectory. Magn Reson Med 55, 575–582 (2006).
6. Cheng JY, Zhang T, Ruangwattanapaisarn N, Alley MT, Uecker M, Pauly JM, Lustig M, Vasanawala SS. Free-breathing pediatric MRI with nonrigid motion correction and acceleration. J Magn Reson Imaging 2015;42:407–420. doi: 10.1002/jmri.24785.
7. Johnson KM, Block WF, Reeder SB, Samsonov A. Improved least squares MR image reconstruction using estimates of k-Space data consistency. Magn Reson Med 2012;67:1600–1608. doi: 10.1002/mrm.23144.
8. Uecker M, Ong F, Tamir JI, Bahri D, Virtue P, Cheng JY, Zhang T, Lustig M. Berkeley Advanced Reconstruction Toolbox. In: 23rd Annual Meeting of ISMRM. Toronto, Ontario, Canada; 2015. p. 2486.
Figures