1022
Accelerated motion compensated 3D isotropic coronary MRA using variable density Cartesian sampling1Division of Imaging Sciences and Biomedical Engineering, King's College London, London, United Kingdom
Synopsis
Accelerated whole-heart 3D isotropic coronary MR angiography (CMRA) is achieved by undersampling the acquisition using a variable-density radial Cartesian (VDRC) trajectory and performing non-rigid respiratory motion correction directly in the low-dimensional-structure self-learning and thresholding (LOST) reconstruction. The proposed approach corrects for 2D beat-to-beat translational and 3D bin-to-bin non-rigid motion. The former is estimated from interleaved image navigators and the latter directly from the CMRA data. The VDRC trajectory provides improved respiratory bin reconstructions and initial image estimate for LOST. The proposed approach produces good quality images, comparable to those of a two-fold accelerated navigator-gated acquisition with ~4x longer scan time.
Introduction
A major challenge in free-breathing whole-heart coronary MR angiography (CMRA) is image degradation due to respiratory motion. Diaphragmatic navigator gating and tracking is commonly used for respiratory motion compensation in CMRA. However, this approach only compensates for superior-inferior (SI) translational motion and scan efficiency is low, leading to prolonged acquisition times as data outside the gating window is rejected. Several methods have been proposed to achieve high scan efficiency and correct for more complex motion in fully sampled acquisitions.1-4 Here we propose to further reduce acquisition time and achieve isotropic resolution by combining a 2D beat-to-beat, image navigators (iNAV) based, intra-bin translational and 3D bin-to-bin non-rigid motion correction approach with a variable-density radial Cartesian (VDRC)5 undersampled acquisition. Undersampled CMRA data are reconstructed using the low-dimensional-structure self-learning and thresholding (LOST)6 approach combined with the generalized matrix formalism (GM), to perform the non-rigid correction directly in the undersampled reconstruction.7,8 The VDRC trajectory is ideal to obtain high quality respiratory-resolved reconstructions from highly undersampled data, essential for accurate estimation of 3D motion parameters using image-based registration. The proposed LOST reconstruction with Cartesian-Ordered acquisition and Motion Correction (LOCOMoCo) was tested on five healthy subjects and compared against a navigator-gated and tracked acquisition.Methods
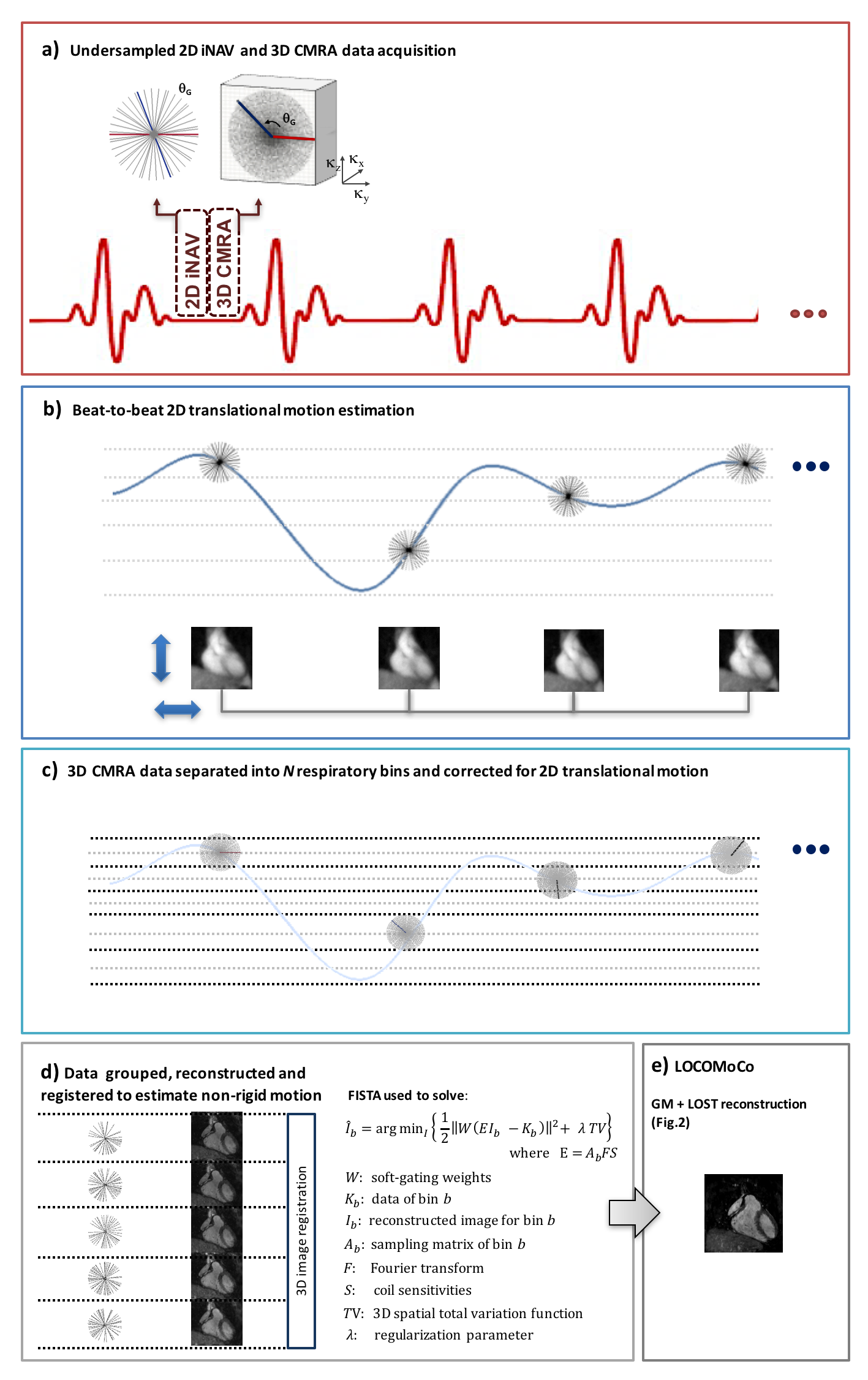
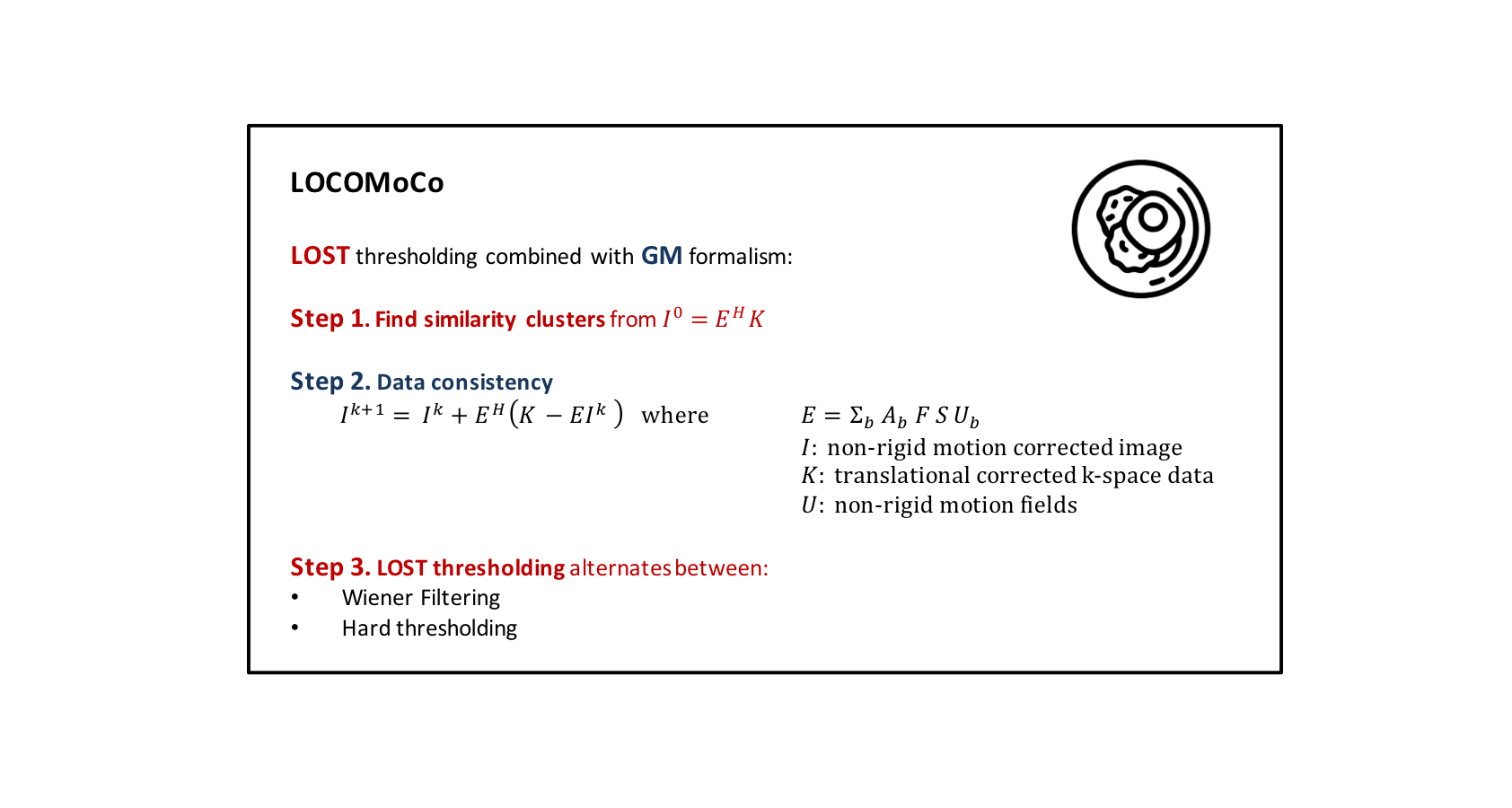
3D CMRA data is acquired using a VDRC trajectory, which samples the ky-kz plane with radial interleaves on a Cartesian grid separated by the golden-angle θG =111.25°. The VDRC trajectory provides denser sampling in the center of k-space, to reduce low-frequency aliasing artifacts due to undersampling, and reduced sensitivity to motion. A 2D golden radial (GR) iNAV is acquired at every heartbeat interleaved with each segment of the whole-heart 3D CMRA scan (Fig1.a). The 2D iNAVs are reconstructed using non-Cartesian SENSE and registered to a common respiratory position to estimate beat-to beat 2D translational (SI and right-left: RL) motion (Fig1.b). The estimated SI motion is used to group the 3D CMRA data into N respiratory bins (Fig1.c) and 2D translational motion correction for each bin is performed in k-space. Each highly undersampled bin is reconstructed using the Fast Iterative Shrinkage-Thresholding Algorithm9 (FISTA) with soft-gating and 3D non-rigid motion is estimated via image registration (Fig1.d). This step is particularly challenging using uniform sampling trajectories due to the high undersampling factors per bin. VDRC sampling facilitates better estimation of 3D motion parameters by allowing higher quality and number or respiratory-resolved bin images. The estimated bin-to-bin non-rigid motion fields are incorporated into an undersampled motion compensated reconstruction using LOCOMoCo (Fig.2). Similarity clusters are learned from zero-filled reconstruction of CMRA data. VDRC fully samples the central k-space region and introduces minimal aliasing artifacts, making the trajectory particularly suitable for this step.
In-vivo free-breathing experiments were performed on five healthy subjects on a 1.5T Philips scanner using a 28-channel receiver coil. Acquisitions were performed using undersampled 2D GR iNAV (gradient echo, 4x4mm in-plane resolution, 25mm slice thickness, 300x300 FOV, TR/TE = 1.9/0.78ms, flip angle = 5°, 24 radial profiles) interleaved with 3D b-SSFP VDRC acquisition. Relevant scan parameters for CMRA are: FOV = 300x300x100mm3, resolution 1.2x1.2x1.2mm3, TR/TE = 5/2.5ms, flip angle = 90°, T2 preparation (50 ms), fat saturation (SPIR), subject specific mid-diastolic trigger delay, acquisition window ~120ms, 1 radial interleaf per R-R interval, 3x undersampling with acquisition time of 5min ± 1.1. Six bins were reconstructed to estimate non-rigid respiratory motion with end-expiration as reference position. A two-fold Cartesian SENSE-accelerated 5mm navigator-gated and tracked acquisition was performed for comparison with acquisition time of 20min ± 2.4. Image quality was assessed by measuring the average vessel length (VL) and sharpness (VS) of both right (RCA) and left (LCA) coronary arteries.
Results
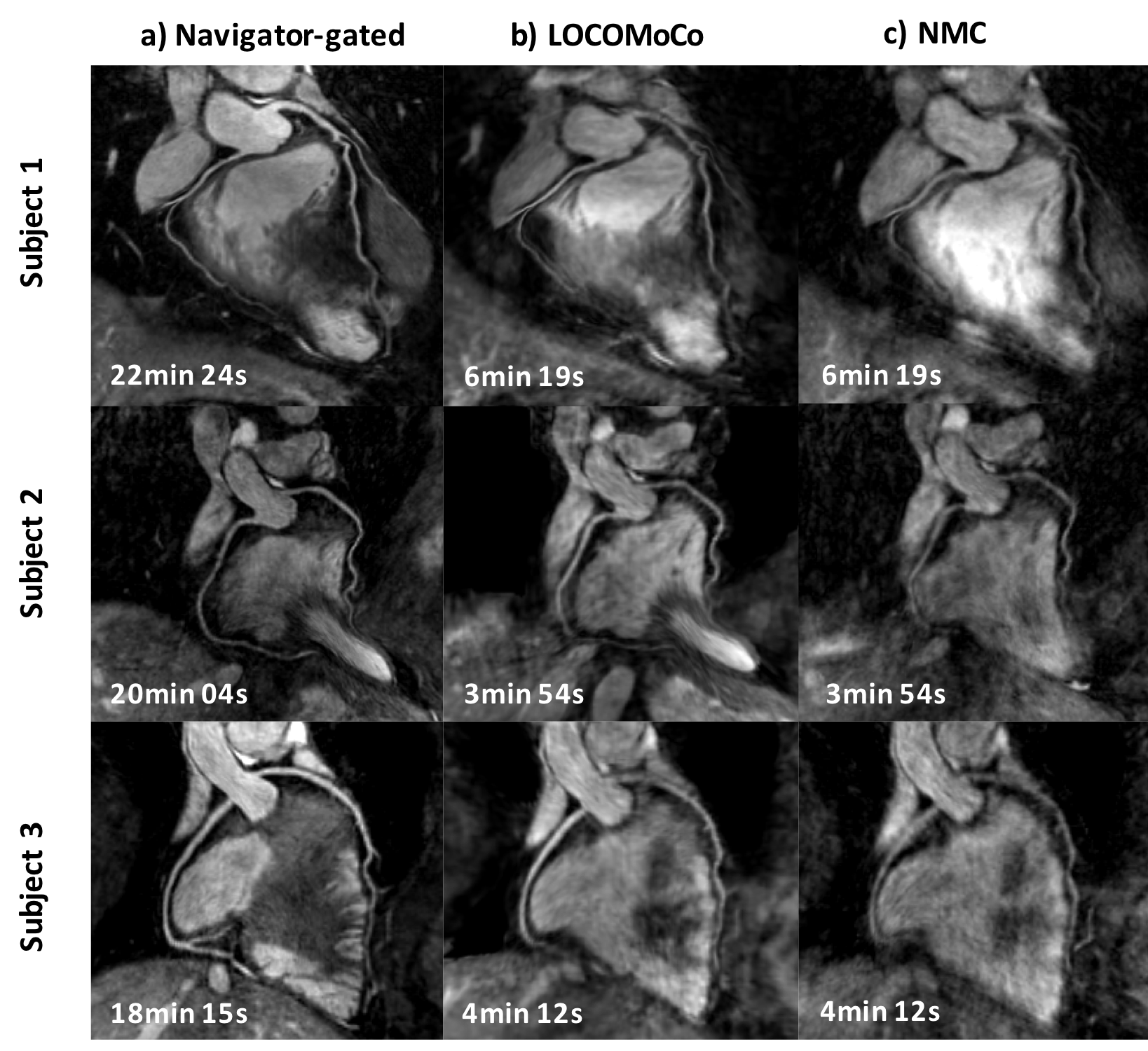
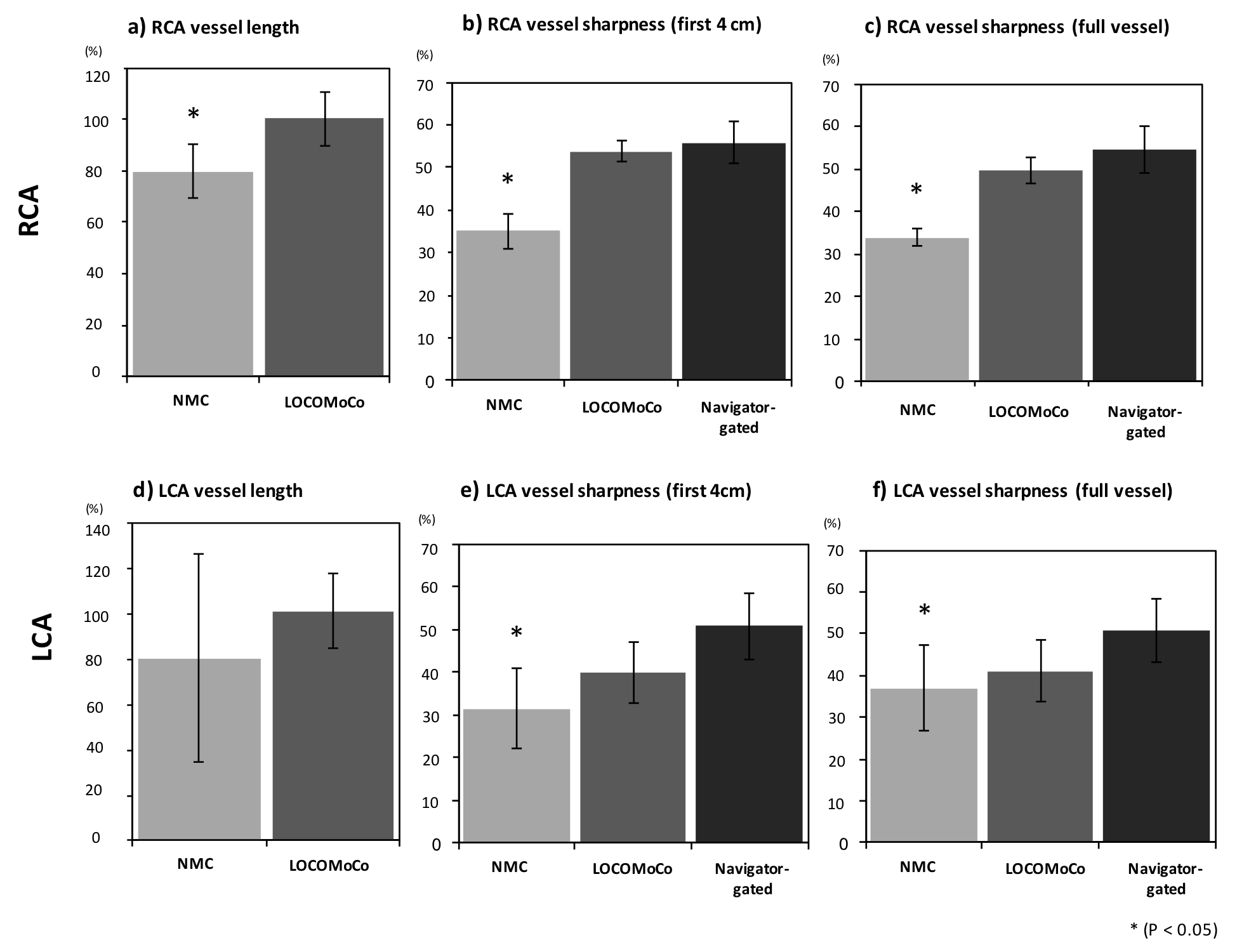
Reformatted images obtained with the proposed LOCOMoCo approach are shown in Fig.3 for three healthy subjects, along with non-motion corrected (NMC) SENSE 3x undersampled reconstructions and navigator-gated two-fold SENSE (in-line reconstructions). Motion blurring is observed in the NMC images. No significant difference in the VL and VS was observed for the RCA between the proposed and the navigator-gated approaches (Fig.4). Slightly reduced image quality (not significant) was observed for the LCA.Conclusions
A highly efficient motion compensated reconstruction framework for accelerated 3D CMRA has been proposed. 2D beat-to-beat translational motion is estimated from iNAVs and 3D non-rigid motion is estimated from undersampled isotropic 3D CMRA. The latter is facilitated by using a VDRC trajectory, which allows high quality bin reconstructions. Non-rigid motion is incorporated into the LOCOMoCo reconstruction, which combines LOST with GM, to obtain images of comparable quality to gated scans, enabling acquisitions to be performed about 4 times faster and with a predictable scan time.Acknowledgements
This work was supported by the Medical Research Council (MRC), grant MR/L009676/1.References
1. Henningsson M, Koken P, Stehning S, et al. Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. MRM 2012; 67:437-445.
2. Bhat H, Ge L, Nielles-Vallespin S, et al. 3D radial sampling and 3D affine transform-based respiratory motion correction technique for free-breathing whole-heart coronary MRA with 100% imaging efficiency. MRM 2011; 65:1269-1277.
3. Aitken A, M Henningsson, Botnar R, et al. 100% Efficient three-dimensional coronary MR angiography with two-dimensional beat-to-beat translational and bin-to-bin affine motion correction. MRM 2014; 74:756-764.
4. Prieto C, Doneva M, Usman M, et al. Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. JMRI 2015; 41:738-746.
5. Cheng J, Zhang T, et al. Free-breathing pediatric MRI with nonrigid motion correction and acceleration. JMRI 2015; 42: 407-420.
6. Akçakaya M, T Basha, Goddu B, et al. Low-dimensional-Structure Self-Learning and Thresholding: Regularization beyond compressed sensing for MRI reconstruction. MRM 2011; 66:756-767.
7. Batchelor P, Atkinson D, Irarrazaval P, et al. Matrix description of general motion correction applied to multishot images. MRM 2005; 54:1273-1280.
8. Cruz G, Atkinson D, Buerger C, et al. Accelerated motion corrected three-dimensional abdominal MRI using total variation regularized SENSE reconstruction. MRM 2016; 75: 1484-98.
9. Beck A, Teboulle M, A
fast iterative shrinkage-thresholding algorithm for linear inverse problems.
SIAM J Imaging Sci 2009; 2: 183-202.
Figures