1021
Silent Navigator-Triggered Silent-MRI in Abdomen1Global MR Applications and Workflow, GE Healthcare Japan, Hino, Japan, 2Office of Radiation Technology, Keio University Hospital, Tokyo, Japan, 3Department of Radiology, Keio University School of Medicine, Tokyo, Japan
Synopsis
We incorporated a silent navigator (sNav) with the whole volume excitation into zero-TE pulse sequence for respiratory motion corrected silent abdominal imaging. The sNav signals showed an excellent correlation between the bellows signals, and resultant zero-TE images had better contrasts than those acquired without respiratory triggering. The sNav-triggered zero-TE technique is expected to be used in abdominal MRI where acoustic noise is problematic (e.g. pediatric patient imaging with anesthesia).
Purpose
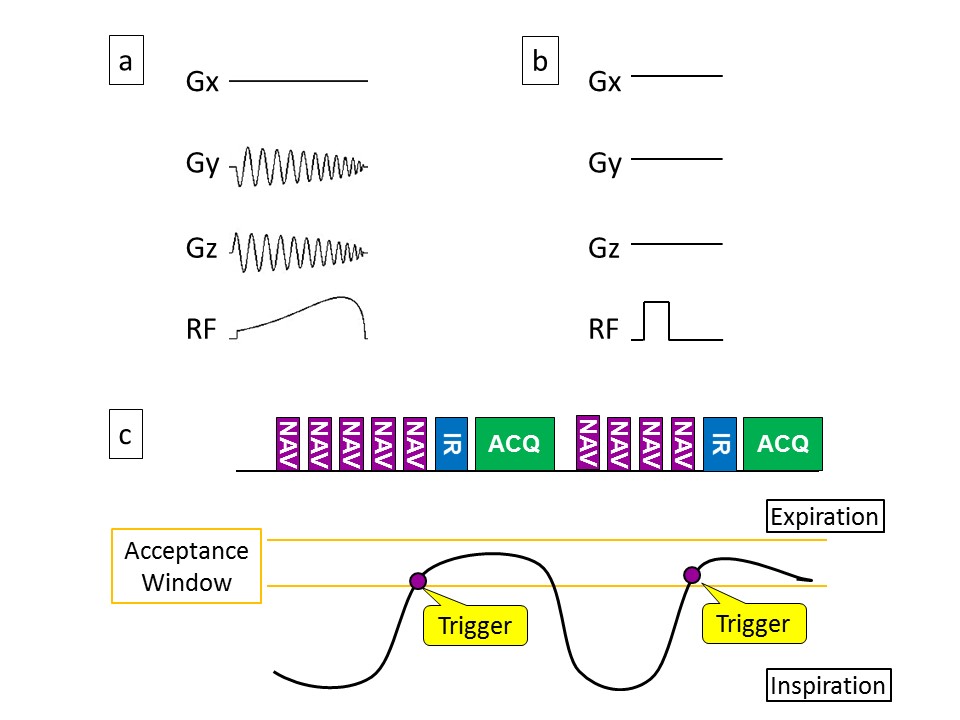
Respiratory navigation with the pencil-beam excitation technique1, 2 is widely used in abdominal MRI, but its oscillating gradient pulses (Fig. 1a) cause large acoustic noise. A navigator technique with the whole volume excitation reduced acoustic noise remarkably while extracting respiratory motion successfully with a proper coil selection.3 In this study, we modified the navigator technique with the whole volume excitation and incorporated it into the zero-TE4 pulse sequence for respiratory motion corrected silent abdominal imaging.Methods
Pulse Sequence: A non-selective hard excitation RF pulse was used without any gradient pulses for not generating high levels of acoustic noise (Fig. 1b), resulting in whole volume excitation. A read-out gradient pulse in the SI direction followed the excitation. Frequency analysis was performed for navigator signals from each coil element, and half of the coil elements with high signal peaks from 0.1 Hz to 0.5 Hz were selected for efficient respiratory motion detection. We refer to this silent navigator method with the whole volume excitation RF pulse as sNav technique. The sNav was incorporated into the silent zero-TE pulse sequence for respiratory triggering; The navigator sequence runs repeatedly and the imaging zero-TE sequence with an inversion recovery (IR) pulse is triggered when the diaphragm position falls within the predefined acceptance window (Fig. 1c). The IR pulse was used for T1-weighted contrast generation.
Data Acquisition: We performed all experiments on a GE 1.5 T MR450w imaging system. The A-weighted continuous equivalent sound pressure level (LAeq) was measured for background, the conventional pencil-beam navigator (pNav), and sNav scans using a Bruel & Kjaer hand-held analyzer type 2270. A microphone mounted in the isocenter of the magnet was connected to the analyzer. Each noise measurement continued for 30 seconds without a receiver RF coil and a phantom. In the pNav and sNav scan, the navigator sequence was repeated every 100 ms during the noise measurement. Navigator-triggered zero-TE scans were performed with six healthy volunteers using a 16-channel phased array coil. The scan was conducted for each navigator technique (pNav/sNav) respectively. Non-triggered free-breathing zero-TE scan (FB) was also conducted for comparison purpose. Imaging parameters in the volunteer scan included: TR/TE = 278.7 ms/0.0 ms, TI = 400 ms, resolution = 2.8 mm, 34 slices, FOV = 36 × 36 cm, NEX = 1, receiver bandwidth = ±26.7 kHz, spokes per segment = 384, and flip angle = 5°. Recovery time = 1000 ms for non-triggered scan.
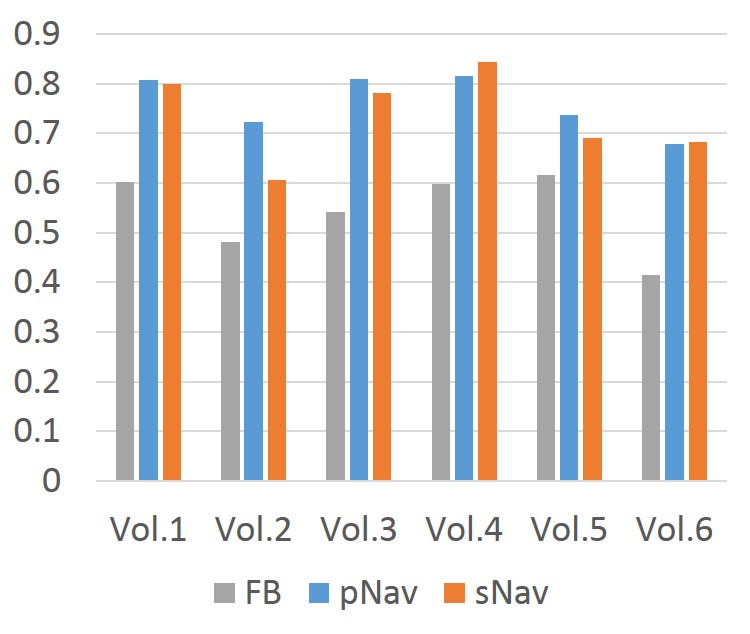
Data Analysis: Correlation coefficients of navigator and bellows signals were calculated for 10-sec learning phase scan where only the navigator sequence runs without imaging components. The relative contrast values5 were calculated by (Sliver-SPV)/(Sliver+SPV) where Sliver is the liver parenchyma signal intensity and SPV is the portal vein signal intensity in the resultant images.Results
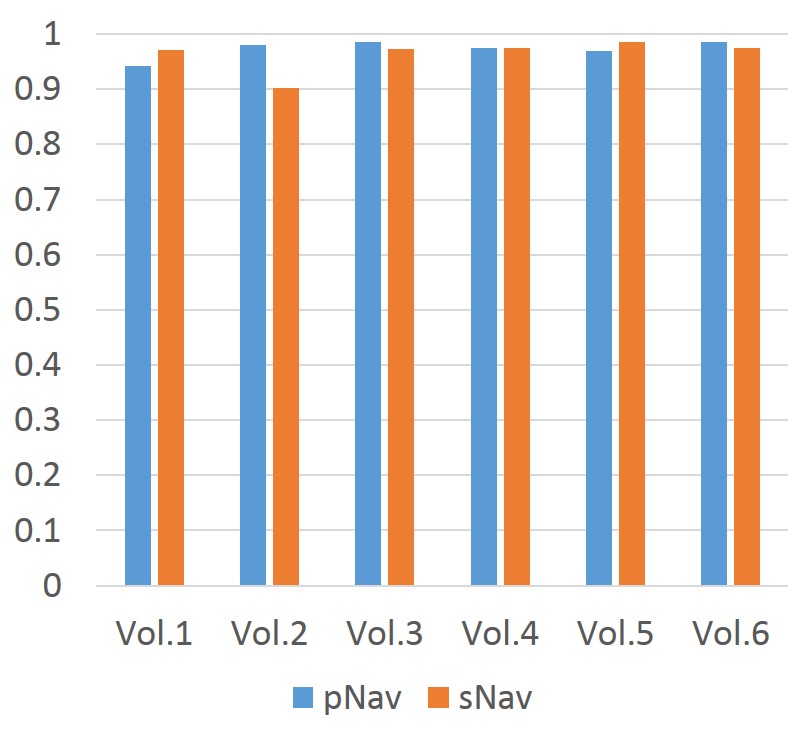
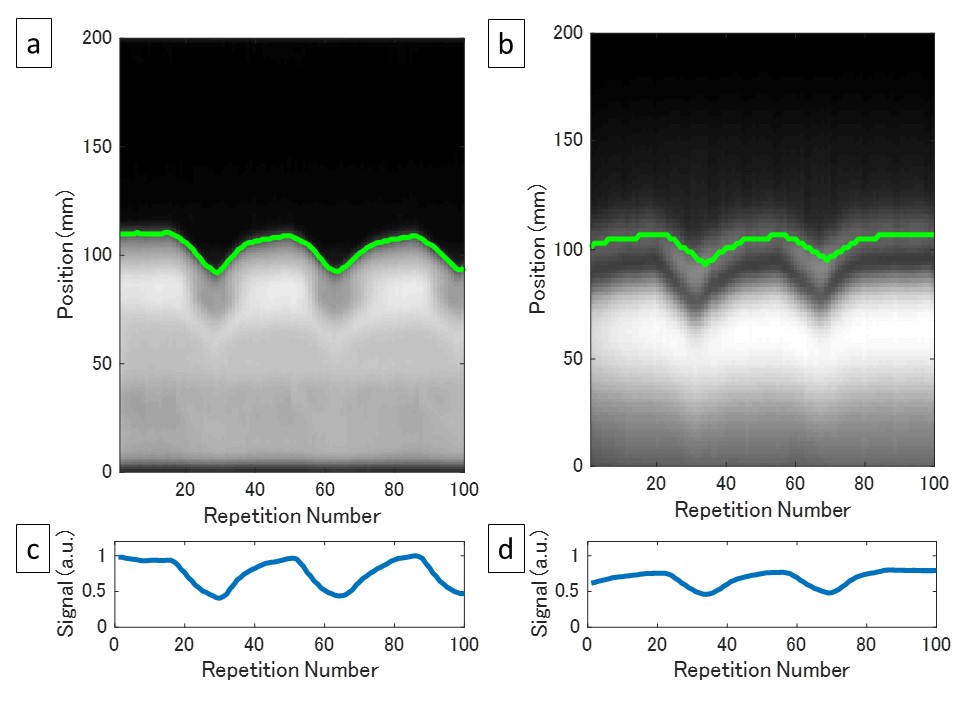
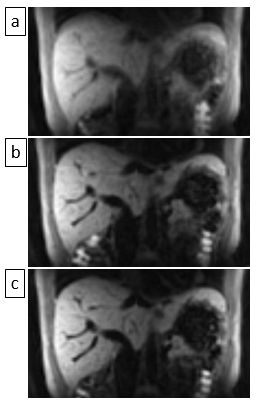
The measured LAeq values of background, pNav and sNav were 67.8 dB(A), 101.5 dB(A) and 69.1 dB(A), respectively, which shows that sNav reduced acoustic noise to almost the same level as background. Fig. 2 shows the correlation coefficients between the bellows signals and calculated displacement values with navigators. All the coefficients are above 0.9 regarding both pNav and sNav, showing the excellent correlation between bellows and navigator signals. Examples of navigator and bellows signals are shown in Fig. 3. The relative contrast values were higher in navigator triggered images with both pNav and sNav than non-triggered images for all subjects (Fig. 4), showing that motion-induced blurring and/or ghosts were decreased with navigators. Differences of the contrast values between pNav and sNav were smaller than 0.05 for five subjects, and the difference was relatively large (0.12) in one subject (Vol.2). Fig. 5 shows examples of zero-TE images acquired in FB, pNav and sNav scans.Discussion and Conclusion
We have demonstrated that combination of the sNav and zero-TE techniques enabled silent respiratory triggered imaging in free-breathing. The results imply that this technique is expected to be used in abdominal MRI where acoustic noise is problematic (e.g. pediatric patient imaging with anesthesia). The contrast between liver and portal vein was worse with sNav than with pNav for one subject (Vol.2). This was due to motion detection imperfection with sNav, probably caused by static tissue signal contamination into navigator signals for whole volume excitation. Modification of the coil combination algorithm such as virtual coil technique6 might improve the accuracy of motion detection. Clinical evaluation with a large number of subjects is required in future.Acknowledgements
No acknowledgement found.References
1. Pauly J, Nishimura
D, et al. A k-space analysis of small-tip-angle excitation. J Magn Reson. 1989;81:43–56.
2. Hardy C, Cline H. Broadband nuclear magnetic resonance pulses
with two-dimensional spatial selectivity. J Appl Phys. 1989;66:1513–1516.
3. Iwadate Y, Nozaki A, et al. Silent navigator with whole volume excitation.
Proceedings of the 24th Annual Meeting of ISMRM, 2016;1856.
4. Madio DP, Lowe IJ.
Ultra-fast imaging using low flip angles and fids. Magn Reson Med.
1995;34:525–529
5. Klessen C, Asbach P, et al. Magnetic resonance imaging of the upper
abdomen using a free-breathing T2-weighted turbo spin echo sequence with
navigator triggered prospective acquisition correction. J Magn Reson Imaging.
2005;21:576–582.
6. Xinwei S, Cheng J, et al. Virtual Coil Navigator: A robust localized
motion estimation approach for free-breathing cardiac MRI. Proceedings of the
23rd Annual Meeting of ISMRM, 2015;811.
Figures