0930
Strain analysis methods from CMR more sensitive than echocardiographic methods to small differences in cardiotoxicity remodeling between risk groups of cancer survivors.1Mechanical Engineering, Polytechnique Montreal, Montreal, QC, Canada, 2Research Center, Montreal Heart Institute, Montreal, QC, Canada, 3Health Center, McGill University, Montreal, QC, Canada, 4Pediatric Oncology, CHU Sainte-Justine, Montreal, QC, Canada, 5Research Center, CHU Sainte-Justine, Montreal, QC, Canada, 6Pediatric Cardiology, CHU Sainte-Justine, Montreal, QC, Canada, 7Kinesiology, Université de Montréal, Montreal, QC, Canada
Synopsis
The use of cardiac strain mapping may provide useful knowledge that may help in detecting doxorubicin-induced cardiotoxicity at a functional scale. Although the feasibility of CMR has been established, there are no standard acquisition protocols or processing pipelines to assess cardiac strain maps. Compared to echocardiography, strain analysis methods from CMR are more sensitive to small differences in cardiotoxicity between risk groups in cancer survivors. While strain mapping from echocardiography remains adequate to detect large differences between healthy volunteers and patients with diseases, our study highlighted the necessity to combine different strain mapping methods to fully describe small cardiac damages
Purpose
Doxorubicin-based chemotherapy is known as an effective treatment for cancer. However, its successes are hindered by its alterations of myocardial physiology at multiple stages, particularly in children who seem more susceptible to these cardiotoxic effects. The use of cardiac strain mapping may provide useful knowledge that may help in detecting doxorubicin-induced damages at a functional scale. Although the feasibility of cardiac magnetic resonance (CMR) has been established, there are no standard acquisition protocols or processing pipelines to assess cardiac strain maps. Methods used to track myocardial displacements include the tagging sequence (1,2), the phase-based strain imaging sequences such as HARP (3) [13] and cine DENSE (4,5), the elastic registration technique (6,7) or contour-based segmentation (8,9). In this study, we investigated 4 different methods of cardiac strain mapping in detecting differences between risk groups of cancer survivors.Methods
We prospectively included 200 survivors of childhood acute lymphoblastic leukemia (cALL), 22.4±6.4 years old, 14.3±5.3 years after the end of treatment, following informed consent and RIB approval of the protocol, and 6 healthy volunteers (HV). Data were analyzed according to cALL prognostic risk groups, standard risk (SR) and high risk (HR), taking into account the administration of dexrazoxane (cardioprotective agent) for the HR group (HRdex). All the survivors underwent a complete echocardiographic assessment including 2D strain analysis based on speckle tracking. A third of the survivors underwent a CMR acquisition including an ECG-gated cine TruFISP sequence at 3T. Myocardial contours were semi-automatically segmented on the mid-ventricular 2-chamber, 4-chamber and short-axis CMR images using an interactive implementation of cubic Bezier curves. The first CMR strain analysis method was a skeleton-based method, in which the internal displacements were interpolated from the contours using kriging. The second CMR strain analysis method was an optical flux method, in which the movement between images was determined based on the gray scale of each pixel considering the conservation of data and the spatial coherence. For the third CMR strain analysis method, an ECG-gated Cine-DENSE-MRI sequence was added to the CMR protocol and the analysis was performed using the “DENSEanalysis” software (5). For all strain data, a one-way analysis of variances was performed.Results
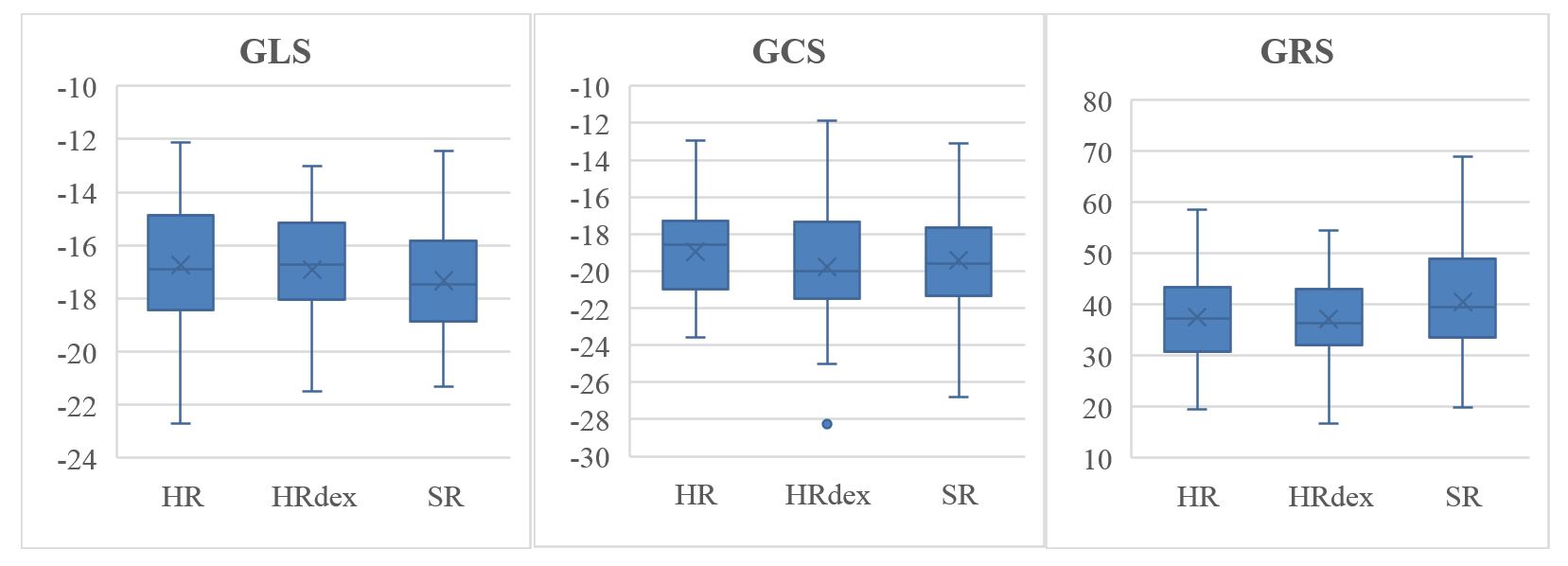
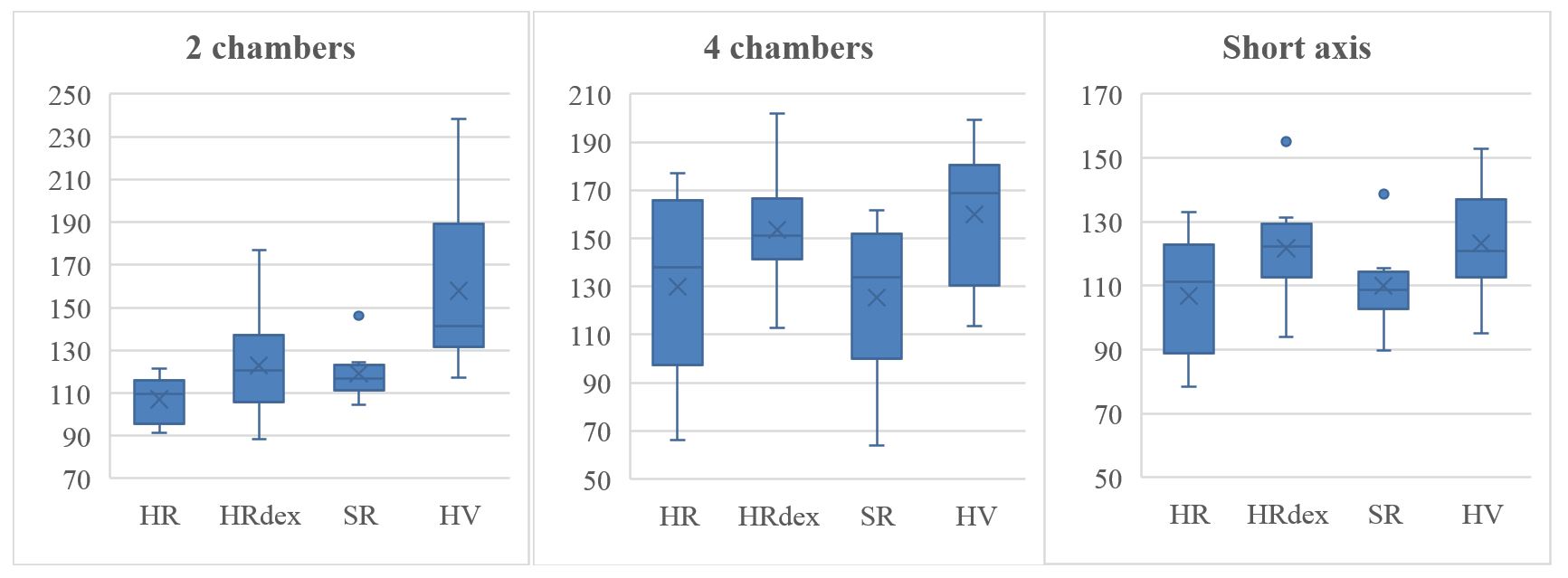
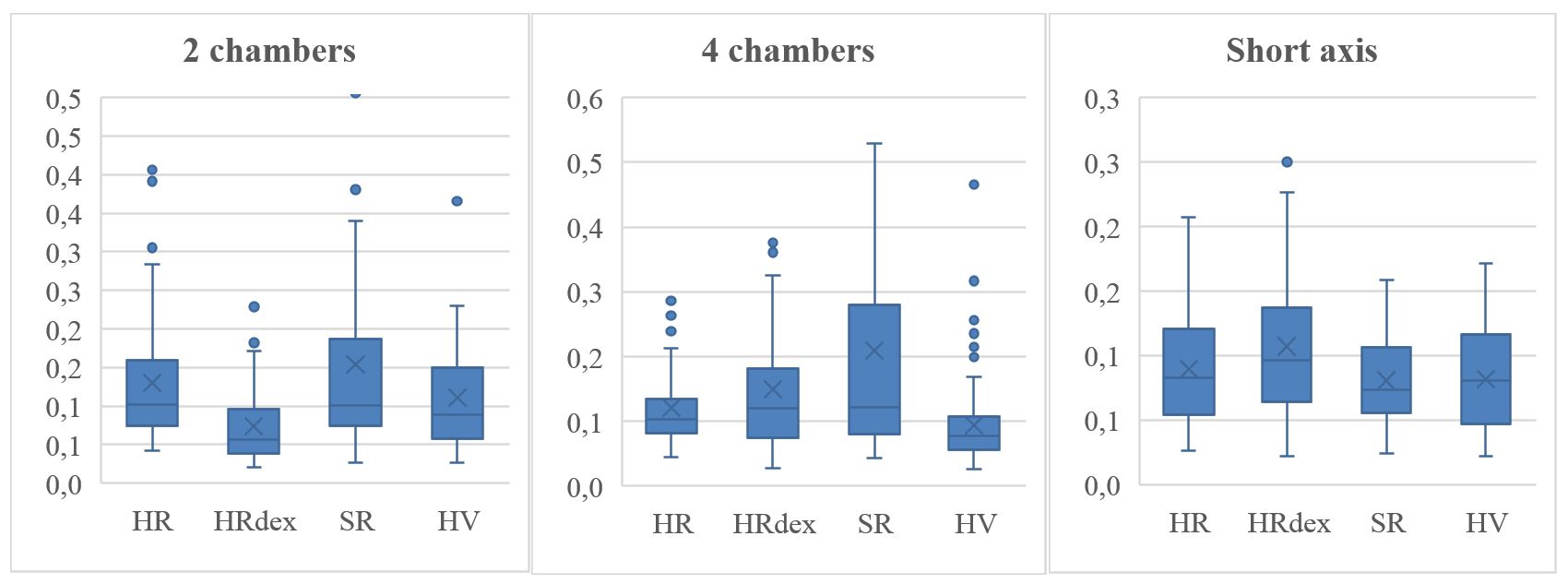
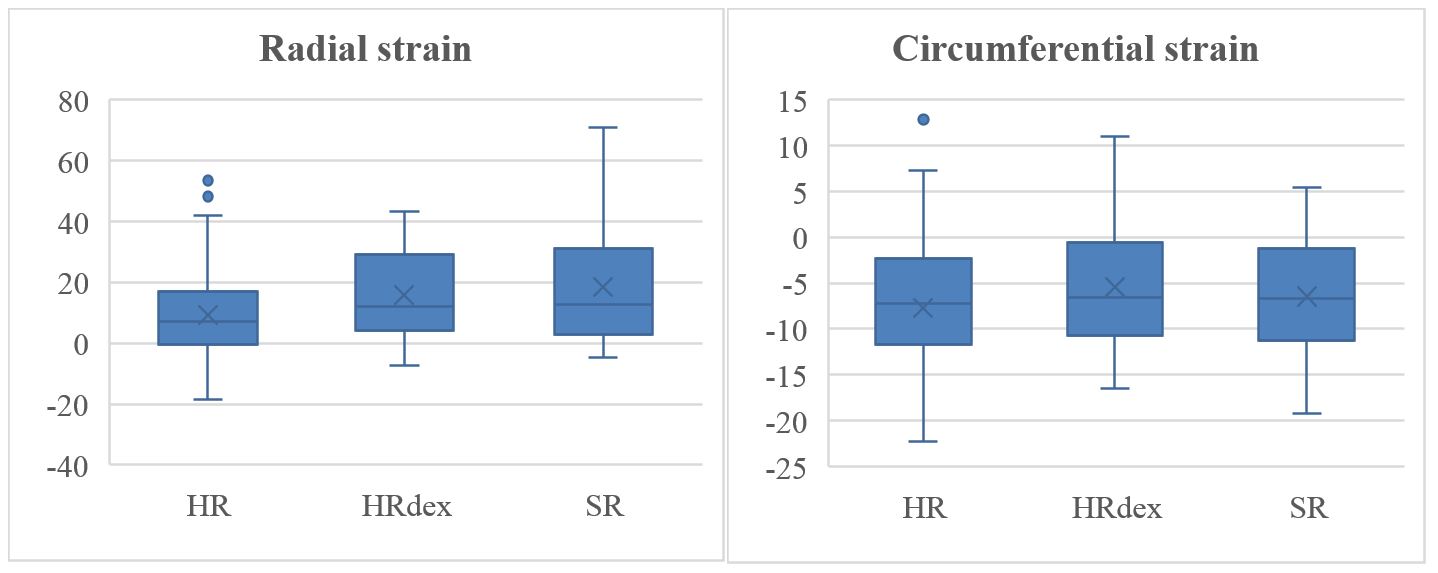
Strain from echocardiography (Figure 1) did not show any differences between cancer survivors (p=0.39, p=0.46 and p=0.10 for global longitudinal, circumferential and radial strain respectively). Strain from the CMR skeleton-based technique (Figure 2) showed differences between healthy volunteers and cancer survivors in the 2 chambers view (p=0.016), but not between cancer survivors risk groups (p>0.1). Strain from the CMR optical flux method (Figure 3) showed differences between HRdex and the other groups in the 2 chambers view (p<0.001), and between HV and the other groups in the 4 chambers view (p<0.001), but no differences in the short axis view (p=0.05). Strain from CMR cine-DENSE (Figure 4) showed differences between HR and SR or HRdex for the radial strain (p<0.001), but no differences for the circumferential strain (p=0.18).Discussion
Each method does not calculate the same strain, leading to different ranges of values. The skeleton-based method cumulates the strain of each phase for all the diastole or systole, leading to higher values, while the cine-DENSE and echocardiographic methods give a global value over the entire cardiac cycle. The optic flux method minimizes the displacement of each pixel at each phase, and a global strain is computed over the systole or diastole, leading to smaller values. While speckle tracking is a robust method to quantify displacements, the lack of sensitivity of the echocardiographic method might be due to the computed global strain, where local strain might be more sensitive. While the CMR acquisition resulted in high quality images, the lack of sensitivity of the skeleton-based method might be due to cardiotoxicity damages located within the cardiac tissue and not at the periphery. However, the CMR skeleton-based method is sensitive lo larger differences, between cancer survivors and healthy volunteers. CMR optic flux and cine-DENSE methods showed different sensitivities, but in different planes of analysis (2-chambers for optic flux, short axis for cine-DENSE).Conclusion
Compared to echocardiography, strain analysis methods from CMR are more sensitive to small differences in cardiotoxicity between risk groups in cancer survivors. While strain mapping from echocardiography remains adequate to detect large differences between healthy volunteers and patients with diseases, our study highlighted the necessity to combine different strain mapping methods to fully describe small differences in cardiotoxicity remodeling between risk groups of cancer survivors so that personalized medicine approach with preventive strategies can be applied and evaluated.Acknowledgements
This work was financially supported by the Cole Foundation (PhD fellowship), the Natural Sciences and Engineering Research Council of Canada (NSERC, Discovery grant and CREATE-MEDITIS Program), the “Fonds de Recherche du Québec en Nature et Technologies” (FRQNT, Team grant) and the Canadian Institute of Health Research (CIHR, team grant).References
1. Young A, Kraitchman DL, Dougherty L, Axel L. Tracking and finite element analysis of stripe deformation in magnetic resonance tagging. IEEE Transactions on Medical Imaging 1995, 14:413-421. 2. Zerhouni EA, Parish DM, Rogers WJ, Yang A, Shapiro EP. Human heart: tagging with MR imaging-a method for noninvasive assessment of myocardial motion. Radiology 1988, 169:59-63.
3. Pan L, Prince JL, Lima JA, Osman NF. Fast tracking of cardiac motion using 3D-HARP. IEEE Trans Biomed Eng. 2005; 52(8):1425-35.
4. Spottiswoode BS, Zhong X, Hess AT, Kramer CM, et al. Tracking myocardial motion from cine DENSE images using spatiotemporal phase unwrapping and temporal fitting. IEEE Trans Med Imaging. 2007;26(1):15-30.
5. Auger DA, Zhong X, Epstein FH, Spottiswoode BS. Mapping right ventricular myocardial mechanics using 3D cine DENSE cardiovascular magnetic resonance. Journal of cardiovascular magnetic resonance 2012; 14:4.
6. Comaniciu D, Zhou XS, Krishnan S. Robust real-time myocardial border tracking for echocardiography: an information fusion approach. IEEE Transactions on Medical Imaging 2004, 23, 849-860.
7. Heyde B, Jasaityte R, Barbosa D, Robesyn V, Bouchez S, Wouters P, Maes F, Claus P, D'hooge J. Elastic image registration versus speckle tracking for 2-d myocardial motion estimation: A direct comparison in vivo. IEEE Transactions on Medical Imaging 2013, 32, 449-459.
8. Comaniciu D, Zhou XS, Krishnan S. Robust real-time myocardial border tracking for echocardiography: an information fusion approach. IEEE Transactions on Medical Imaging 2004, 23: 849-860
9. Wang V, Hoogendoorn C, Engelbrecht G, Frangi A, Young A, Hunter P, Nash M, 2012. Unsupervised segmentation and personalised FE modelling of in vivo human myocardial mechanics based on an MRI atlas. 9th IEEE International Symposium on Biomedical Imaging (ISBI) 2012, pp1360-1363.
Figures