0919
The use of 3D FSE in place of 2D T2-FSE, 2D T2*-GRE in the diagnosis of cervical spinal non-neoplastic lesion1MR application, GE healthcare china, shanghai, People's Republic of China, 2radiology, Chinese medicine hospital of Linyi, shandong, People's Republic of China, 3radiology, the second affiliated hospital of Shandong university of traditional Chinese medicine, shandong, People's Republic of China, 4radiology, the second hospital of Shandong university, shandong, People's Republic of China, 5MR modality, GE healthcare china, beijing, People's Republic of China
Synopsis
Magnetic resonance imaging has been accepted as the predominant imaging tool for diagnosis of spinal disease, such as protrusion of intervertebral disc, tumor, inflammation, trauma [1]. T2 weighted imaging is commonly used for diagonosis in many medial centers, however 2D fast spin echo (FSE) image quality is often limited by several practical factors including low fat content, high susceptibility effect and vunerability to motion and pulsation. T2* weighted imaging is another popular choice [2]. Improved contrast may be obtained between gray matter and white matter of medullar. The drawback of T2* imaging is the hyperintense gray matter signal may may cause the small cervical spinal cord lesion to be overlooked. In this work, the use of 3D FSE is assessed and compared to 2D T2 and T2* imaging, and hypothesized to overcome their shortcomings.
Purpose
Magnetic resonance imaging has been accepted as the predominant imaging tool for diagnosis of spinal disease, such as protrusion of intervertebral disc, tumor, inflammation, trauma [1]. T2 weighted imaging is commonly used for diagonosis in many medial centers, however 2D fast spin echo (FSE) image quality is often limited by several practical factors including low fat content, high susceptibility effect and vunerability to motion and pulsation. T2* weighted imaging is another popular choice [2]. Improved contrast may be obtained between gray matter and white matter of medullar. The drawback of T2* imaging is the hyperintense gray matter signal may may cause the small cervical spinal cord lesion to be overlooked. In this work, the use of 3D FSE is assessed and compared to 2D T2 and T2* imaging, and hypothesized to overcome their shortcomings.Methods
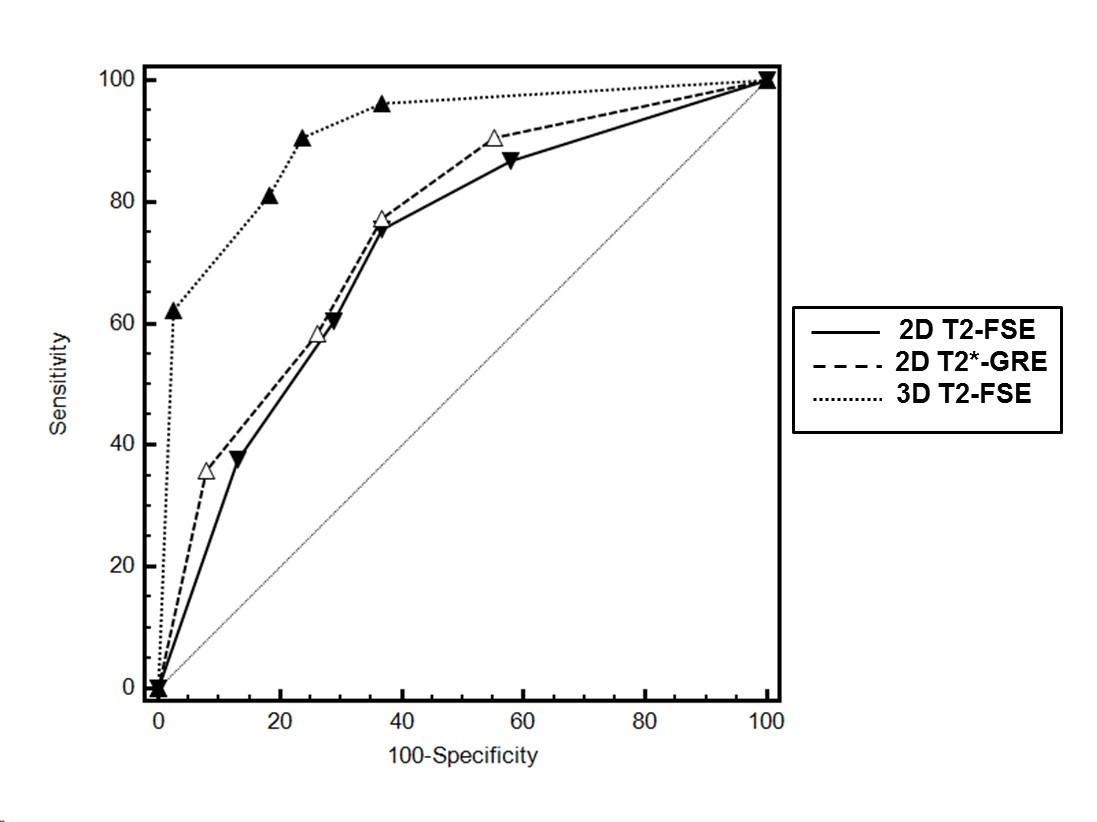
A total of 53 patients with clinical symptoms (24 men, 29 women, age 43±9 ) and 25 healthy controls (13 men, 12women, 19–73 years old, mean age 41±13) were enrolled in this study and content forms were obtained prior to the study. The clinical symptom included sensory disturbance, depressed muscular tension, tendon hyporeflexia, respiratory muscle paralysis, acroparalysis, etc. All cases were later confirmed by cilinical diagnosis. MR scans were performed on a 3.0T whole body scanner (Discovery MR 750, GE, USA). Axial 2D T2-FSE, 2D T2*-GRE, 3D T2-FSE, and sagittal sagittal short tau inversion recovery (STIR) images were obtained for all participants: axial 2D T2-FSE, TR/TE=4000ms/100ms, ETL=16; axial 2D T2*-GRE, TR/TE= 500ms/12ms; axial 3D T2-FSE, TR/TE=4000ms/100ms, ETL=50; STIR, TR/TE=4000ms/100ms, ETL= 16, TI=200ms. Two experienced radiologists reviewed and graded the images using a 5 points scale : grade 1 normal, grade 2 approximately normal, grade 3 suspicious, grade 4 approximately abnormal, grade 5 abnormal. Statistical analysis was calculated by the Medcal software package. ROC curve graph was drawn. Diagnostic efficiency was compared by AUC ( area under curve ).Results
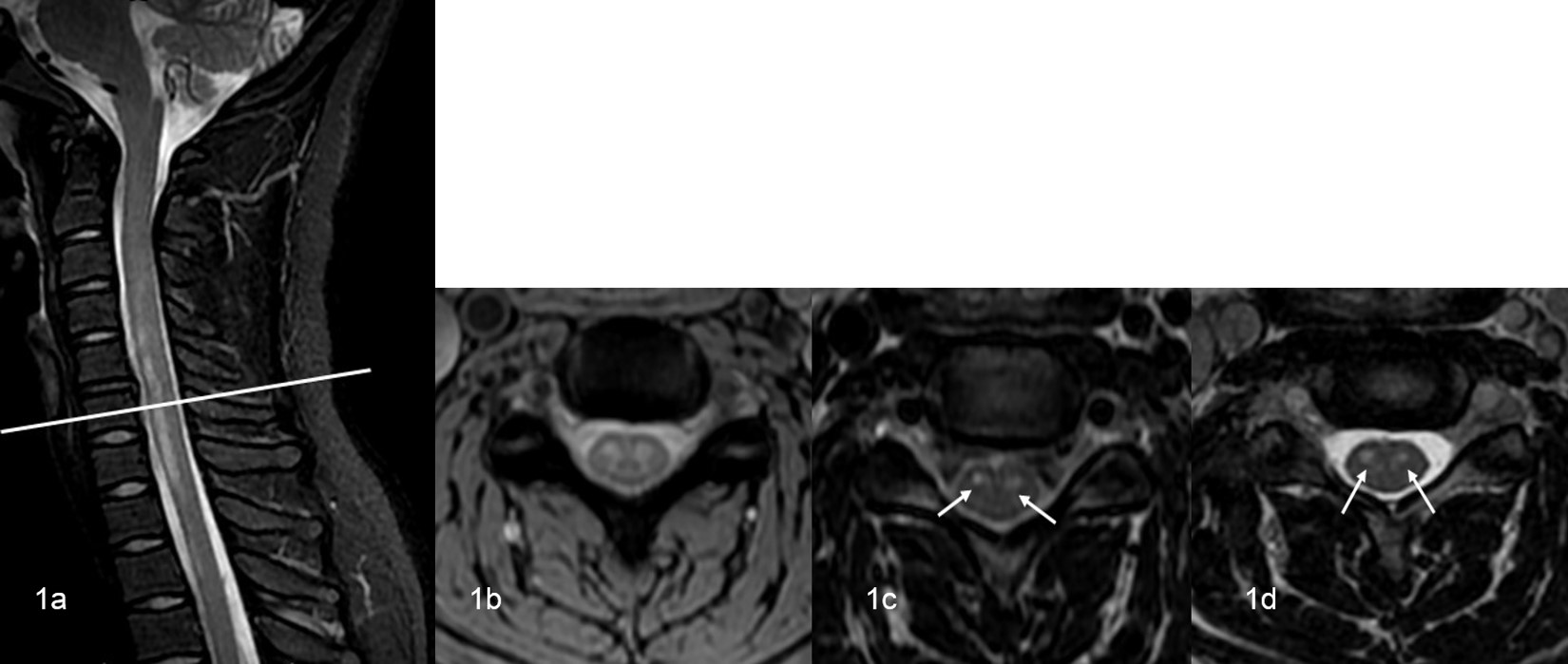
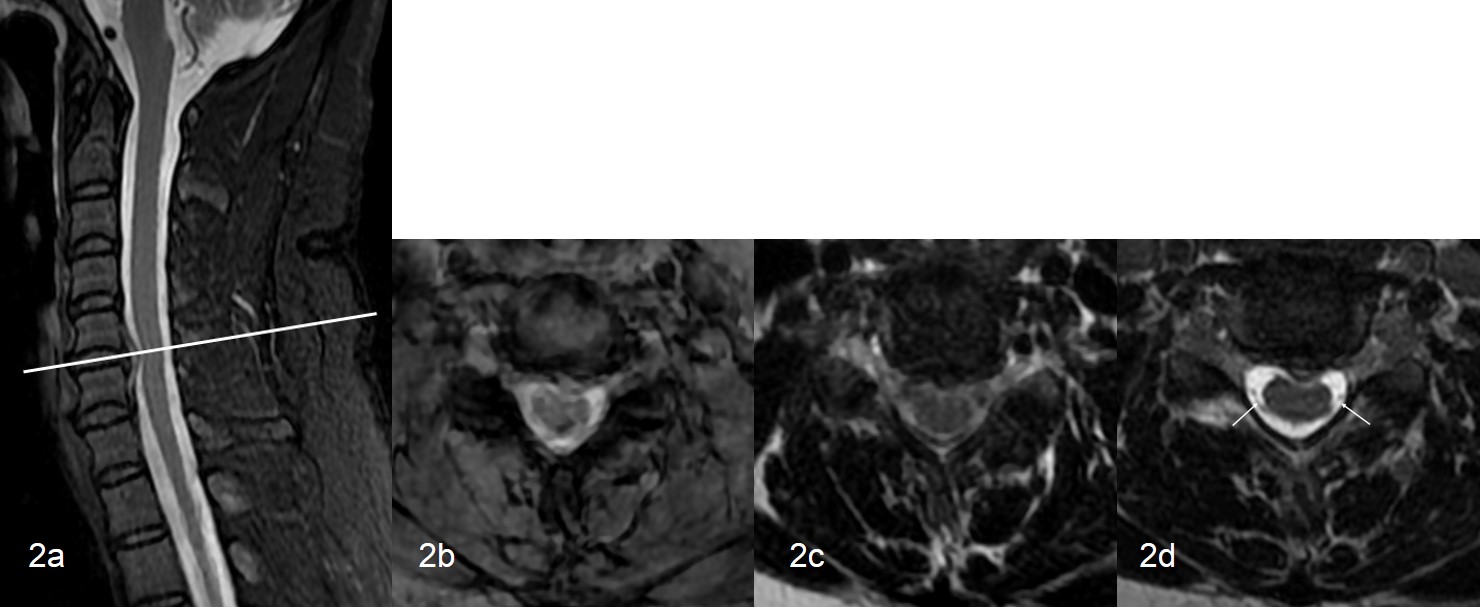
Out of 53 cervical spinal non-neoplastic cases, there were 5 cases of transvers myelitis, 8 cases of Guilain-Barre syndrome, 10 cases of radiation myelitis, 13 cases of demyelination, 17 cases ofcervical spinal degeneration generated by protrusion of intervertebral disc. Images of a Guilain-Barre syndrome case are shown in Fig.1, where the lesion was overshowed by the gray matter contrast in T2*. Another case with intervertebral disc protrusion is shown in Fig.2, and in this case the both 2D GRE and 2D FSE was deteriorated by motion artifacts due to CSF flow and pulsation. The AUC of 2D T2-FSE、2D T2*-GRE and 3D T2-FSE is 0.720, 0.753 and 0.909, respectively; 95% CI ( confidence interval ) of 2D T2-FSE、2D T2*-GRE and 3D T2-FSE is 0.616 to 0.809, 0.652 to 0.838, 0.830 to 0.959, respectively.Discussion and conclusion
Both 2D GRE and FSE have been widely used for diagnosis of spinal diseases. However they both feature their own shortcomings, as demonstrated in this study : 2D GRE may lead to masked intramedullary lesion by hyperintense gray matter signal; the 2D FSE is vunerable to through-plane CSF flow and pulsation artifacts. 3D FSE, on the other hand, has not yet been widely accepted in clinical routine imaging for spinal diseases. It has been demonstrated in this study that 3D FSE is qualitatively advantageious to both 2D GRE and 2D FSE. Furthermore, in the corhort study it was shown that 3D FSE feature a higher AUC than 2D FSE and 2D GRE. Hence 3D FSE may have high clinical potential in observing leisons related to spinal cord, intraspinal nerve roots, neural foramen, foraminal fat, vertebral bone, intervertibral disc, and facet joints.Acknowledgements
No acknowledgement found.References
1 Visveshwar B, F.Scott P, Eric J R, Etl. Myelographic MR imaging of the cervical spine with a 3D true fast imaging with steady-state precession technique: initial experience [J]. Radilogy, 2003, 227(2): 585-592.
2 T. Meindl, S. Wirth, S. Weckbach, Etl. Magnetic resonance imaging of the cervical spine: comparison of 2D T2-weighted turbo spin echo, 2D T2* weighted gradient-recalled echo and 3D T2-weighted variable flip-angle turbo spin echo sequences [J]. Eur Radiol,2009, 19(3): 713-721.
Figures