0903
Image quality assessment for free-breathing dynamic liver examination using a self-navigated Cartesian acquisition with iterative reconstructionBenjamin Kaltenbach1, Dominik Nickel2, Ralph Strecker2, Andreas Bucher1, Thomas J. Vogl1, and Boris Bodelle1
1Goethe University Frankfurt, Frankfurt, Germany, 2Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
Free-breathing DCE-MRI of the liver is feasible using a Cartesian acquisition with self-navigation and hard-gated reconstruction in oncological patients. Compared to a standard BH-VIBE, image quality was rated marginally lower but with useful robustness regarding breathing artifacts. Therefore, the proposed sequence is a promising alternative in patients who cannot comply with breathing commands, like children or elderly patients.
Introduction
Dynamic contrast enhanced magnetic resonance imaging (DCE-MRI) of the liver represents an important fundament for the identification and characterization of liver lesions. As liver DCE-MRI is generally acquired using breathholds (BHs), respiratory artifacts are a frequent source for image quality degradation, especially in patients with limited BH-capacity. An emerging strategy to address this problem is the use of continuous free-breathing acquisitions with iterative reconstruction [1,2]. The purpose of the present proof-of-concept study was an image quality comparison between a prototypical free-breathing Cartesian VIBE acquisition with self-navigating signal and hard-gated reconstruction [3] and a conventional BH-VIBE as image quality gold standard in oncologic patients.Methods
Seventeen consecutive patients (mean age 59 ± 11 years, 45% female, mean BMI 26±4kg/m2) underwent continuous free-breathing dynamic liver imaging using a prototypical self-navigated Cartesian VIBE sequence as part of their oncologic follow-up (FOV: 380x344mm2; image matrix: 320x218; TE: 1.8ms; TR: 3.76ms; slice thickness: 3mm; flip angle: 10°; 16 time points with a temporal resolution of 11.57s each, gating acceptance 40%; Figure 1). The free-breathing approach was compared to the patient’s last standing dynamic liver MRI including a standard BH-VIBE (FOV: 325x400mm2; image matrix: 320x195; TE: 1.26ms; TR: 3.97ms; slice thickness: 3mm; flip angle: 9°; acceleration mode: CAIPIRINHA) which served as institutional diagnostic gold standard. Examinations were performed on a clinical 3T scanner (MAGNETOM PrismaFit, Siemens Healthcare, Erlangen, Germany). In a first session, best arterial and venous phase were determined by one radiologist for the free-breathing reconstruction. After this, overall image quality, liver edge sharpness, hepatic vessel clarity, visibility of retroperitoneal structures and breathing artifacts were scored retrospectively, blindly and independently by two additional radiologists using a 5-point Likert scale with highest score indicating best image quality. Image quality parameters were compared using a paired Wilcoxon test with a p-value <0.05 considered as statistically significant. The mean value of native, arterial and venous phases was taken into account.Results:
Both sequences presented with diagnostic quality standard (Figure 2). The free-breathing sequence showed slightly lower quality scores for overall image quality (4.2±0.5 vs. 4.4±0.4; p<0.05) and liver edge sharpness (3.9±0.5 vs. 4.2±0.6; p<0.05), whereas both hepatic vessel clarity (4.4±0.8 vs. 4.3±0.7; p=0.22) and visibility of retroperitoneal structures (4.5±0.5 vs. 4.5±0.4; p=0.45) were scored with same high quality as standard BH-VIBE. Both sequences presented with comparable respiratory artifacts (3.9±0.8 vs. 3.8±0.6; p=0.33). Reconstruction time for the free-breathing sequence was 9 ± 1min.Discussion:
Our preliminary results indicate that free-breathing DCE-MRI using a Cartesian sequence with self-navigating signal and hard-gating motion correction is feasible in oncologic patients. The proposed sequence can represent a promising alternative in patients who cannot comply with breathing commands, like children or elderly patients. The reconstruction time is passable and therefore integrable in daily clinical routine. Indeed, the high temporal resolution is an advantage for arterial contrast pattern to discriminate between early and late enhancement but regarding venous phases, the main advantage relies in an increase of motion robustness as several comparable venous phases are available and the number of equivalent reconstructions with diagnostic quality is high.Acknowledgements
No acknowledgement found.References
[1] Feng L et al, MRM 72(3), 2014
[2] Zhang T et al, JMRI 41(2), 2015
[3] Nickel D et al, #4253, ISMRM 2016
Figures
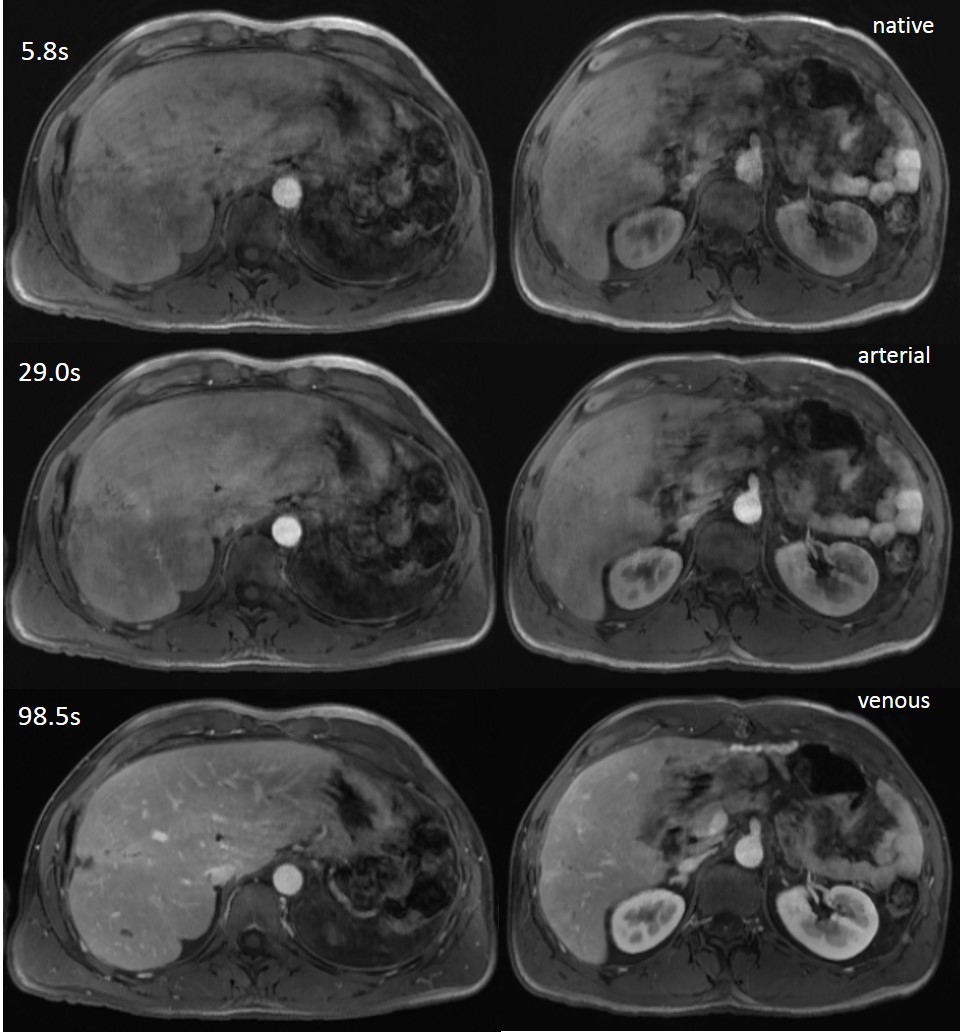
Free-breathing
Cartesian sequence with hard-gated reconstruction and a gating tolerance of 40%
for native (after 5.8s) and for best rated arterial (after 29.0s) and venous
phase (after 98.5s).
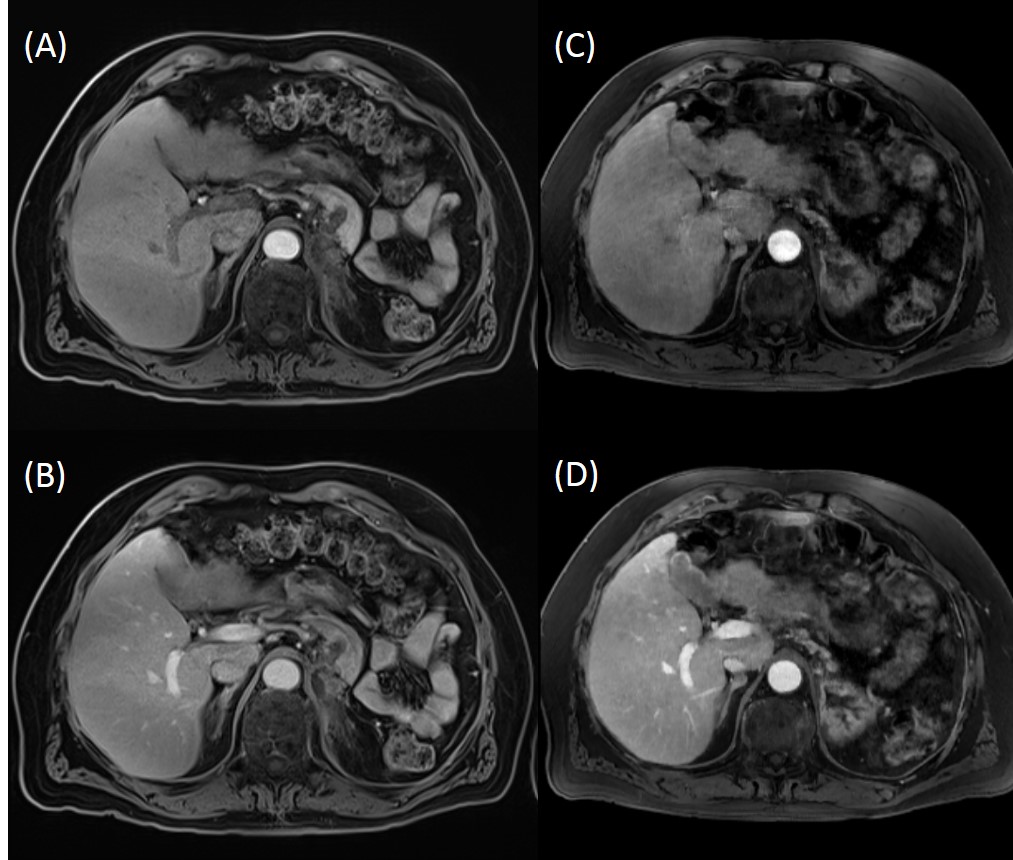
Intraindividual
comparison of BH (A, B) and free-breathing (C, D) VIBE close to the liver hilus
for arterial and venous reconstruction in a 64-year old patient with known
liver metastases.