0900
Quantitative susceptibility mapping in the neonatal brain with congenital heart disease1Division of Diagnostic Imaging and Radiology, Children’s National Medical Center, Washington, DC, United States, 2Division of Fetal and Transitional Medicine, Children’s National Medical Center, Washington, DC, United States, 3Departments of Radiology and Pediatrics, George Washington University, Washington, DC, United States, 4Division of Cardiology, Children’s National Medical Center, Washington, DC, United States
Synopsis
Brain injury is a frequent complication in newborns with complex congenital heart disease (CHD) secondary to hemodynamic instability and increased risk for hypoxic-ischemic injury. In this study quantitative susceptibility mapping (QSM) was performed in newborns with complex CHD prior to open heart surgery and was compared to healthy control newborns. Mean susceptibility was significantly higher in the cortical gray matter of neonates with CHD versus controls suggesting reduced oxygenation in the cerebral vasculature in CHD preoperatively. QSM images also depicted less contrast in the CHD, which may be associated with delayed brain development. This is the first report to demonstrate the feasibility of neonatal QSM and susceptibility differences between CHD and controls.
INTRODUCTION
Congenital heart disease (CHD) is the most common type of birth defect associated with significant mortality and morbidity, and the potential for lifelong brain injury and neurodevelopmental dysfunction among surviving infants. Increasing evidence suggests that preoperative cerebral oxygen delivery is reduced in the neonatal brain with specific CHD1-3. Quantitative susceptibility mapping (QSM) is an emerging tool used to measure magnetic susceptibility of tissue, which can be directly related to venous oxygenation when measured within veins4-6. In this study we performed QSM in the neonatal brain with CHD and demonstrated a significant difference in susceptibility compared to healthy controls.METHODS
Five neonates diagnosed with CHD and 14 healthy control neonates were recruited in the context of a separate prospective study. MR phase imaging was performed using a 3D multi-echo flow-compensated gradient echo sequence with imaging parameters of TR = 55 ms, TE = 5.8, 12.2, 18.6, 25.0, 31.4, 37.8, 44.2 ms, BW = 50 kHz, flip-angle = 20°, FOV = 16 cm, and spatial revolution of 0.38 x 0.5 x 2 mm3. Total scan time was 6:09 min with parallel imaging (acceleration factor=2). All MRI scans were performed on a GE MR 750 3T scanner using an 8-channel head coil while the infants were breathing room air. QSM reconstruction was performed using the approach of morphology-enabled dipole inversion (MEDI)7. Estimated susceptibility maps were registered to T2-weighted images of the same subject using rigid-body image registration with SPM (Wellcome Trust Center for NeuroImaging, UCL, UK) and then registered to the templates of the neonatal brain using nonrigid-body registration with ANTS (http://stnava.github.io/ANTs). Brain regions were segmented using the Draw-EM neonatal atlas (https://github.com/MIRTK/DrawEM). All other analysis was performed using Matlab (MathWorks, Natick, MA).RESULTS
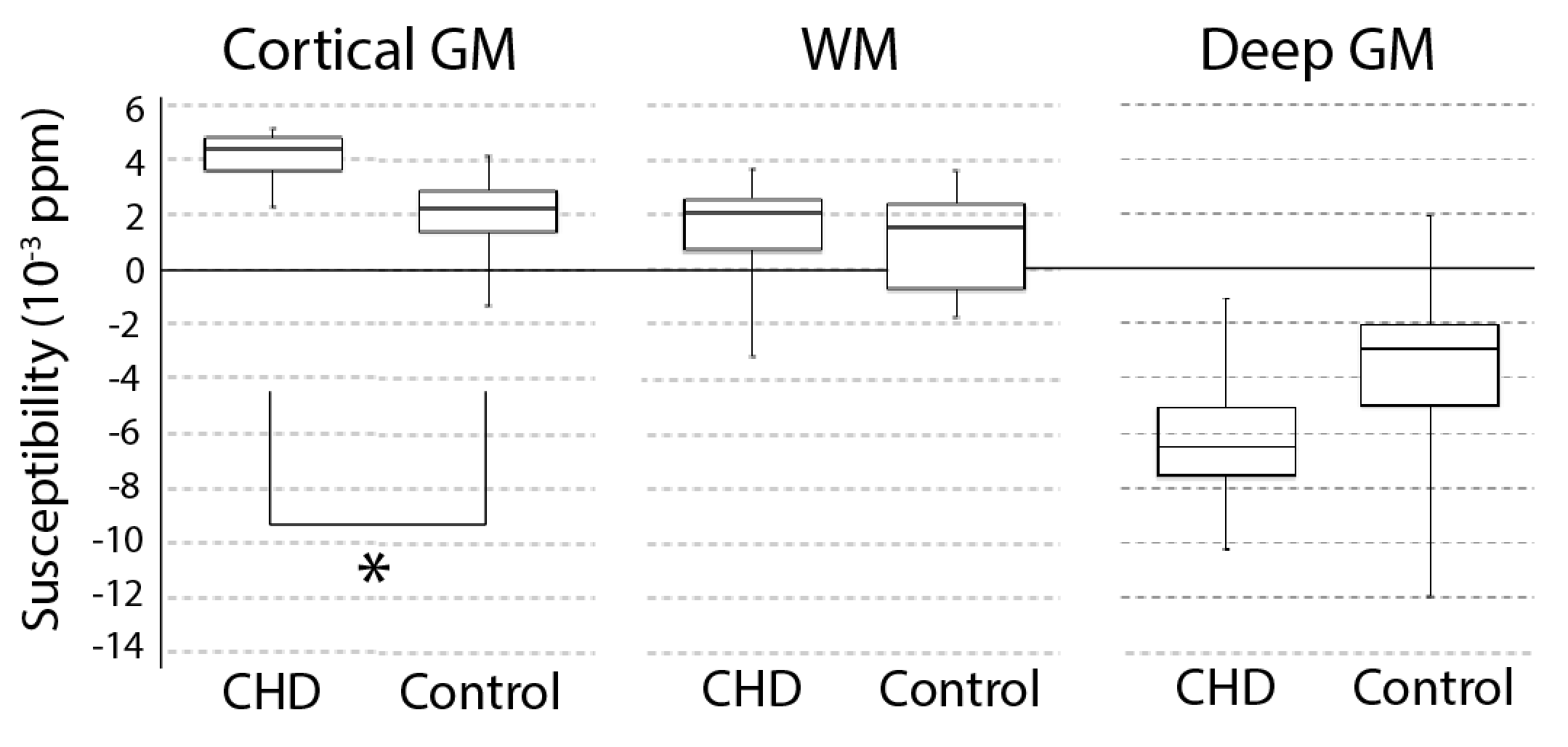
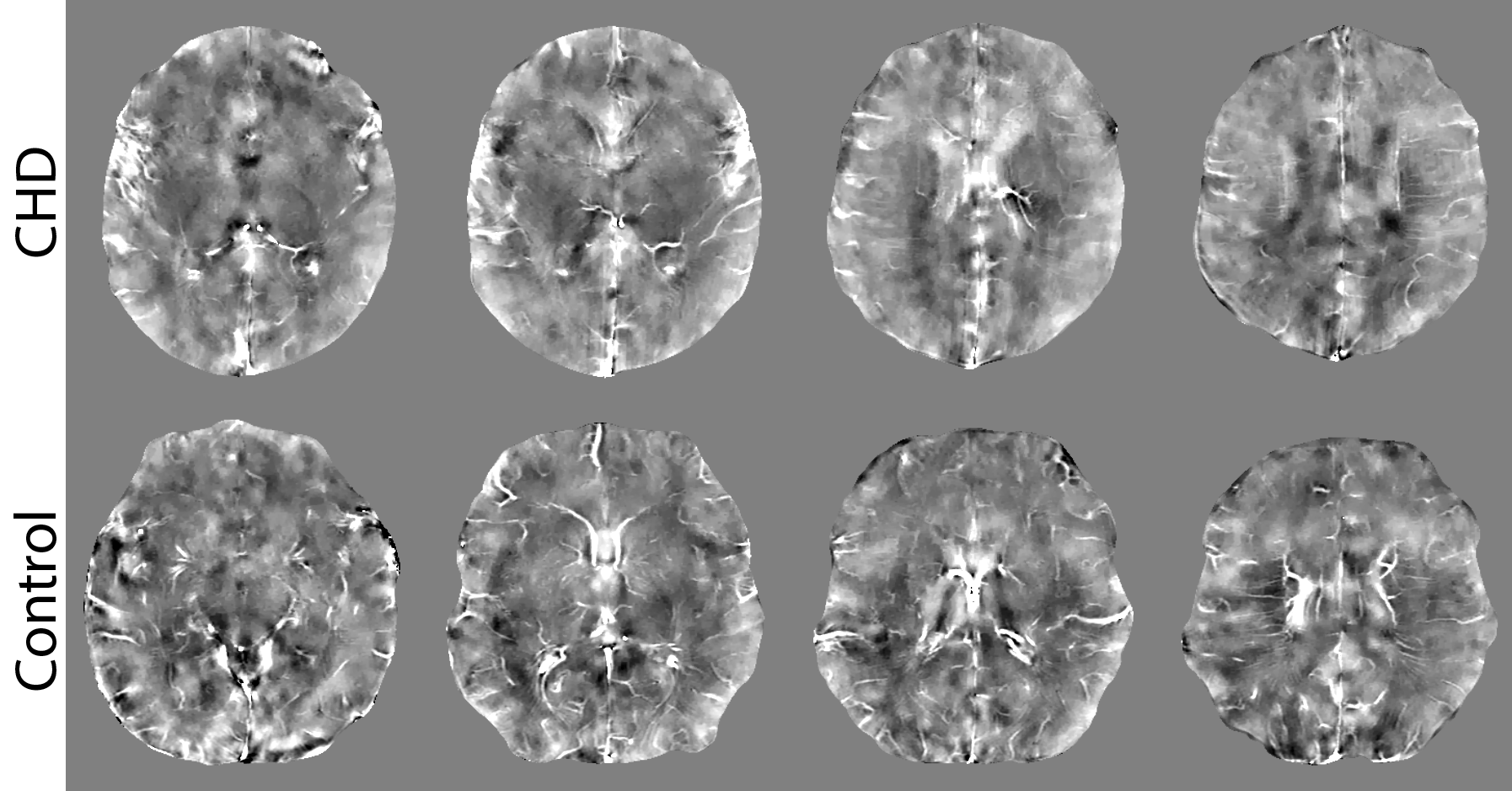
One neonate with CHD and 1 healthy neonate were excluded from the analysis due to image artifacts caused by subject motion during MR image acquisition. Data from the remaining 4 neonates with CHD and 13 healthy neonates were used for QSM analysis. Mean age at the time of MRI scan was 7±12 days for CHD and 14±8 days for healthy neonates (p=0.11). Cardiac diagnoses included ventricular septal defect, hypoplastic left heart syndrome, d-transposition of the great arteries, and truncus arteriosus. Measured mean susceptibility was 40±13 vs 20±14 in the cortical gray matter, 12±30 vs 11±17 in the white matter, and -61±38 vs -38±40 in the deep gray matter for CHD vs healthy controls, respectively (all in unit of 10-4 ppm). Figure 1 shows the box and whisker plot of measured susceptibility in the three regions. Among those regions, only cortical gray matter showed a significant difference in susceptibility between CHD and controls when controlling for age (p=0.02). Figure 2 shows QSM images of representative infants (one CHD and one control) and demonstrates increased cortical gray matter susceptibility in the infant diagnosed with CHD. In addition, the healthy infant showed greater spatially variant contrast representing more developed brain structure than the infant with CHD. Unlike adult brain, the neonatal brains showed no hyperintensity in the basal ganglia on QSM images due to insufficient iron deposition.DISCUSSION
We demonstrate the feasibility of performing QSM in neonates and report a significant increase in cortical gray matter susceptibility in neonates with CHD prior to open heart surgery compared to healthy controls. To the best of our knowledge, this is the first report of neonatal brain QSM. Increased susceptibility in the cortical gray matter may be attributed to reduced oxygenation (i.e. increased deoxyhemoglobin content) in the venous and capillary vasculature. Future studies will evaluate direct estimation of oxygen saturation with measurement of susceptibility in large cerebral veins.Acknowledgements
No acknowledgement found.References
1. Licht DJ, Wang J, Silvestre DW, et al. Preoperative cerebral blood flow is diminished in neonates with severe congenital heart defects. J Thorac Cardiovasc Surg. 2004;128:841-849.
2. Lim JM, Kingdom T, Saini B, et al. Cerebral oxygen delivery is reduced in newborns with congenital heart disease. J Thorac Cardiovasc Surg. 2016;152:1095-1103.
3. Nagaraj UD, Evangelou IE, Donofrio MT, et al. Impaired Global and Regional Cerebral Perfusion in Newborns with Complex Congenital Heart Disease. J Pediatr. 2015;167:1018-1024.
4. Fan AP, Bilgic B, Gagnon L, et al. Quantitative oxygenation venography from MRI phase. Magn Reson Med. 2014;72:149-159.
5. Xu B, Liu T, Spincemaille P, et al. Flow compensated quantitative susceptibility mapping for venous oxygenation imaging. Magn Reson Med. 2014;72:438-445.
6. Haacke EM, Tang J, Neelavalli J, et al. Susceptibility mapping as a means to visualize veins and quantify oxygen saturation. J Magn Reson Imaging. 2010;32:663-676.
7. Liu J, Liu T, de Rochefort L, et al. Morphology enabled dipole inversion for quantitative susceptibility mapping using structural consistency between the magnitude image and the susceptibility map. Neuroimage 2012;59:2560–2568.
Figures