0895
White matter diffusion properties at term equivalent age are associated with subsequent motor performance in infants born preterm1Centre for the Developing Brain, Division of Imaging Sciences & Biomedical Engineering, King's Collge London, London, United Kingdom, 2Centre for Medical Image Computing, Department of Computer Science, University College London, London, United Kingdom, 3Neonatal Unit, St Georges Hospital NHS Trust, London, United Kingdom
Synopsis
Preterm birth is associated with a high prevalence of neuro-motor impairment. We studied the relationship between motor function at two years and DTI measures in white matter (WM) fasciculi at term equivalent age using tract specific analysis in 109 preterm infants. Motor performance was significantly positively correlated with FA and negatively correlated with RD and MD in the corticospinal tract (CST) and corpus collosum (CC). DTI measures in other tracts were not related to motor function, suggesting a specific relationship between WM in the CST and CC and motor ability in this vulnerable group.
Purpose
Brain development is adversely affected by preterm birth and motor impairment is prevalent in this population1. Early therapeutic intervention is beneficial to motor outcome2 and so identification of infants at risk in the neonatal period is key. Our aim was to study the association between diffusion tensor imaging (DTI) measures in specific fasciculi at term-equivalent age and motor outcome at two years using tract-specific analysis (TSA)3. TSA creates skeleton models of specific fasciculi onto which diffusion data can be projected for statistical analysis. This offers the benefits of anatomically specific analysis with the ability to highlight regions of statistical significance at locations along a tract.Methods
Subjects: We studied 109 infants (59 male) born between 25.7-32.9 (median 30.1) weeks gestational age (GA) and imaged at 40.0-41.9 (median 41.1) weeks postmenstrual age (PMA). Infants were recruited as part of the E-Prime study of preterm brain development, written parental consent was obtained prior to imaging. Motor performance was assessed using Bayley Scales for Infant and Toddlers Development (BSID-III) at two years.
MRI Acquisition: MR imaging was performed on a 3T MR system on the neonatal intensive care unit. Single shot echo planar diffusion-weighted MRI was acquired in 32 non-collinear directions with parameters; TR=8000 ms, TE=49 ms, slice thickness 2mm, voxel size: 2mm3 isotropic, b-value=750s/mm2, SENSE factor of 2. T1- and T2-weighted MR imaging were also acquired.
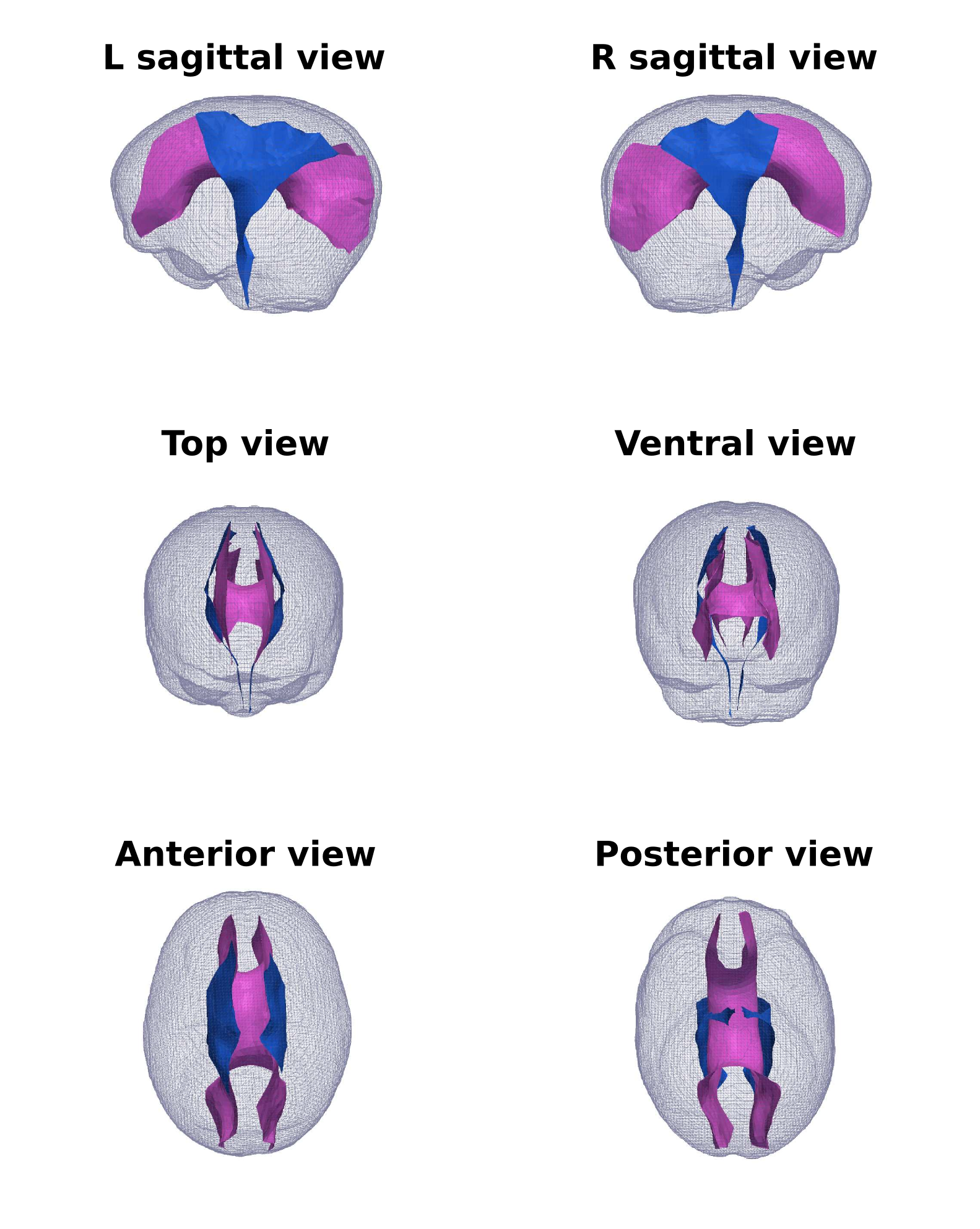
TSA framework: A subset of 20 subjects without focal lesions were registered to create an iteratively-refined, study-specific template using a tensor-based algorithm4. The remaining 89 subjects were registered to this template. WM tracts were delineated in the template using deterministic tractography with manually drawn regions of interest5. We studied the corpus callosum (CC), corticospinal tract (CST), inferior fronto-occipital fasciculus (IFOF), inferior longitudinal fasciculus (ILF) and uncinate fasciculus (UNC). Each tract was modeled as a medial surface – the tract skeleton, with a tract boundary6. Diffusion data from every subject was projected onto the skeleton by searching within the tract boundary along the unit normal from the skeleton to the boundary. Regression analysis was carried out at each vertex on the skeleton between fractional anisotropy (FA), axial, mean, and radial diffusivities (AD, RD, MD) and composite motor scores. Covariates in the model were GA, PMA, gender and whether the infant was used to generate the template. To correct for family-wise errors, non-parametric permutation-based suprathreshold cluster analysis was performed with primary threshold of p=0.05.
Results
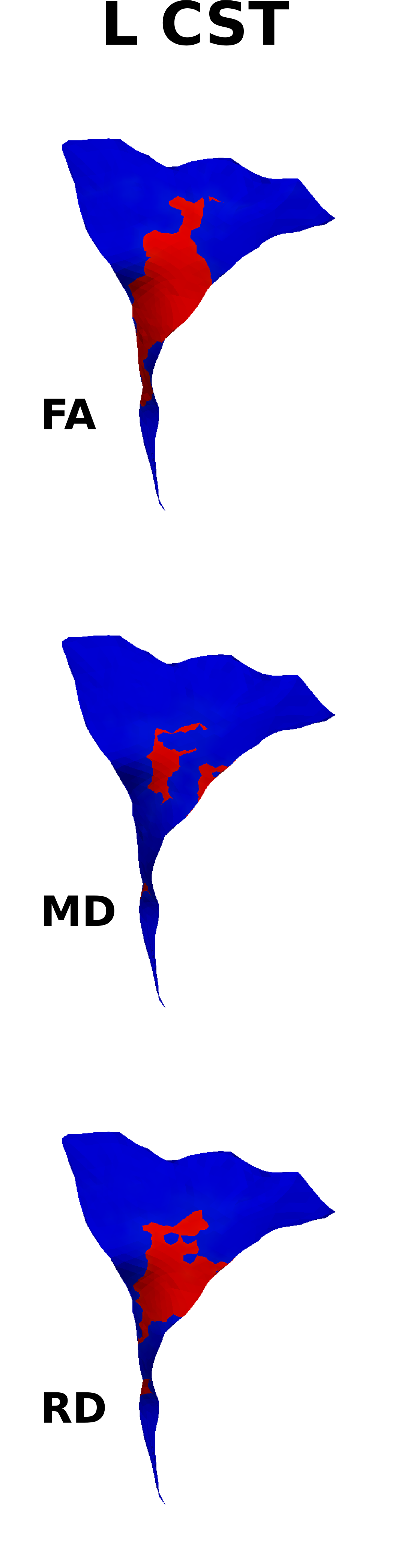
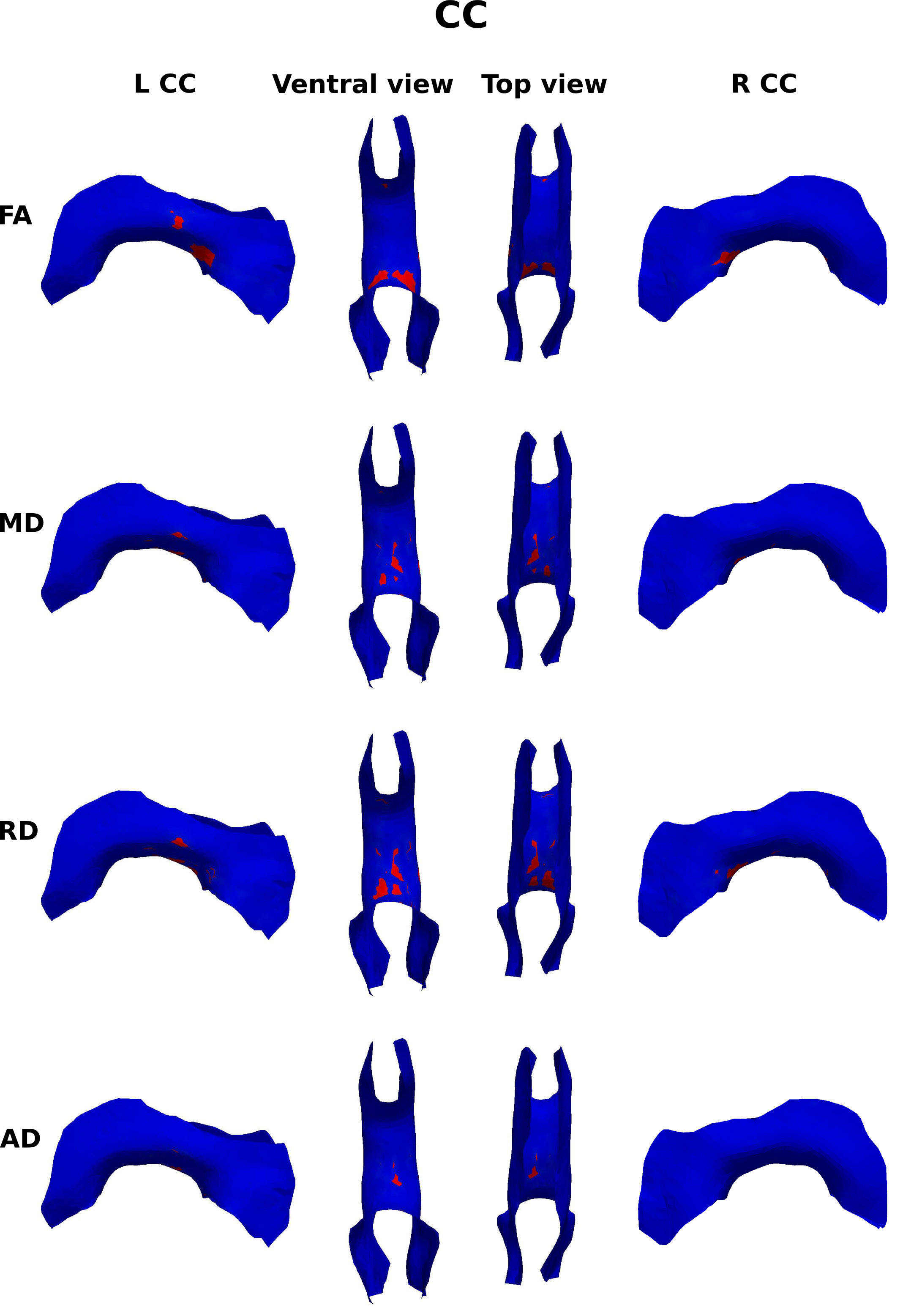
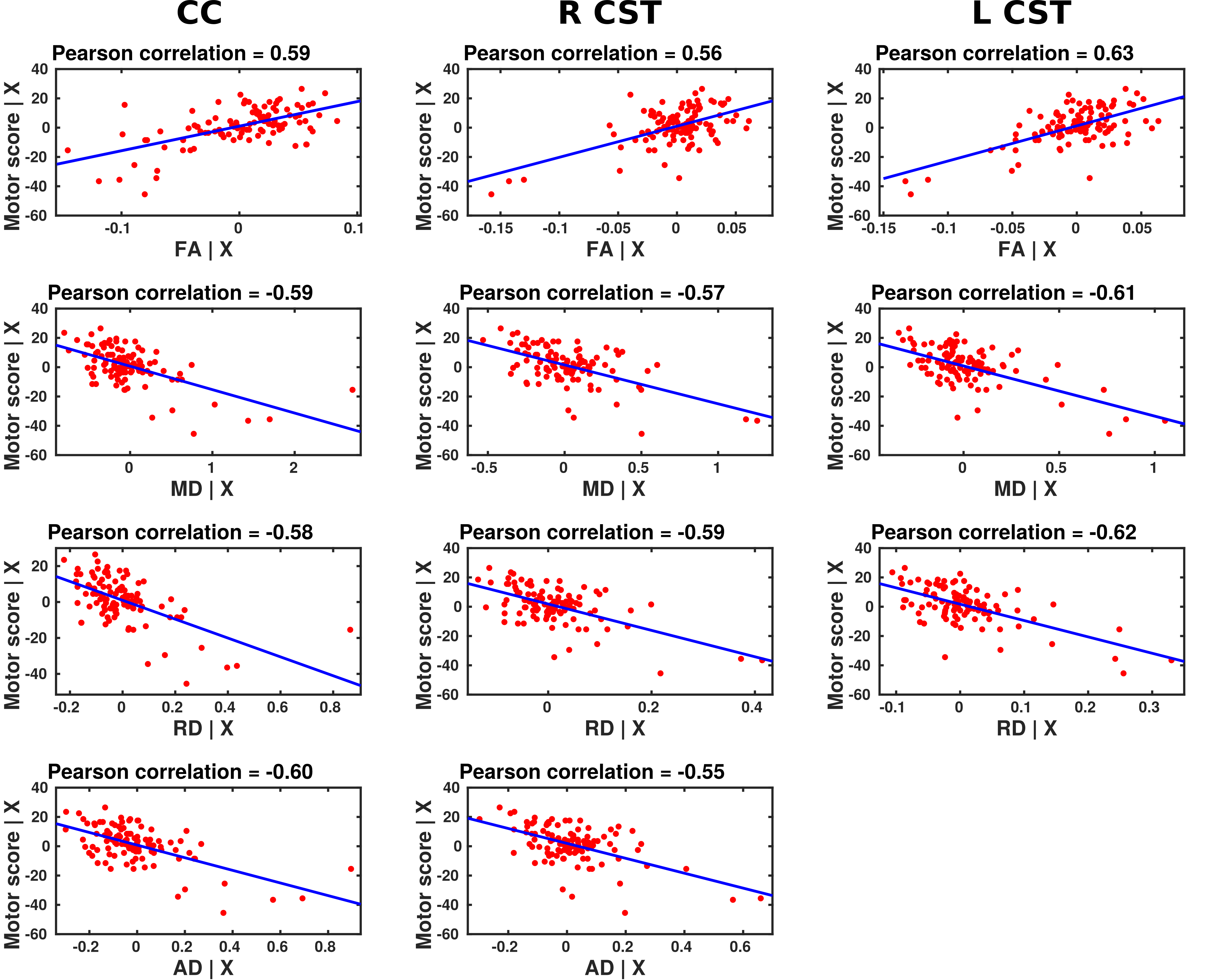
The median motor score for the infants was 97 (range 46-118). Results from the TSA model fitting for the CC and CST are shown in figure 1. Motor scores were significantly positively correlated with FA in the splenium of the CC and in the CST bilaterally; negatively correlated with RD and MD in the body of the CC and in the CST bilaterally; and negatively correlated with AD in the right CST (figures 2-5). No correlation was found between motor score and DTI measures in any of the other tracts.Discussion and Conclusion
Using TSA we were able to assess a number of different WM fasciculi across a large sample of preterm infants. We identified tracts in which DTI measures in the neonatal period correlated to motor function at two years; the CST and the body and splenium of the CC. While previous diffusion tractography studies have shown FA values in the CST and CC are associated with subsequent motor function in the preterm population, these studies did not explore other WM fasciculi7. Here we show the relationship with performance is specific to these tracts. The ability to determine at an early age which WM fasciculi are associated with motor ability in childhood offers the potential to identify infants at risk and who may benefit from appropriate therapeutic intervention.Acknowledgements
This study was funded in part by the National Institute for Health Research and the Medical Research Council.References
1. Williams, J., Lee, K. J. & Anderson, P. J. Prevalence of motor-skill impairment in preterm children who do not develop cerebral palsy: a systematic review. Dev Med Child Neurol 52, 232-237, doi:10.1111/j.1469-8749.2009.03544.x (2010).
2. Hughes, A. J., Redsell, S. A. & Glazebrook, C. Motor Development Interventions for Preterm Infants: A Systematic Review and Meta-analysis. Pediatrics, doi:10.1542/peds.2016-0147 (2016).
3. Yushkevich, P. A., Zhang, H., Simon, T. J. & Gee, J. C. Structure-specific statistical mapping of white matter tracts. Neuroimage 41, 448-461, doi:10.1016/j.neuroimage.2008.01.013 (2008).
4. Zhang, H., Yushkevich, P. A., Alexander, D. C. & Gee, J. C. Deformable registration of diffusion tensor MR images with explicit orientation optimization. Med Image Anal 10, 764-785, doi:10.1016/j.media.2006.06.004 (2006).
5. Wakana, S. et al. Reproducibility of quantitative tractography methods applied to cerebral white matter. Neuroimage 36, 630-644, doi:10.1016/j.neuroimage.2007.02.049 (2007).
6. Yushkevich, P. A. & Zhang, H. G. Deformable modeling using a 3D boundary representation with quadratic constraints on the branching structure of the Blum skeleton. Inf Process Med Imaging 23, 280-291 (2013).
7. De Bruine, F. T. et al. Tractography of white-matter tracts in very preterm infants: a 2-year follow-up study. Dev Med Child Neurol 55, 427-433, doi:10.1111/dmcn.12099 (2013).
Figures