0893
Characterising white matter tracts of the limbic system and neurodevelopmental outcomes in children born very preterm1Murdoch Childrens Research Institute, Melbourne, Australia, 2Department of Paediatrics, The University of Melbourne, Melbourne, Australia, 3Florey Institute of Neuroscience and Mental Health, Melbourne, Australia, 4The Florey Department of Neuroscience and Mental Health, The University of Melbourne, Melbourne, Australia, 5Department of Neurosurgery, The Royal Children's Hospital, Melbourne, Australia, 6Neuroscience Research, Murdoch Childrens Research Institute, Melbourne, Australia, 7Developmental Imaging, Murdoch Childrens Research Institute, Melbourne, Australia, 8Neonatal services, Royal Women’s Hospital, Melbourne, Australia, 9Department of Obstetrics and Gynaecology, The University of Melbourne, Melbourne, Australia
Synopsis
Children born very preterm are at risk of having problems with memory, learning, behavioural and emotional functioning, which are key functions of the brain’s limbic system. In 144 very preterm compared with 33 full-term 7-year-olds, altered microstructure, including axon density and orientation dispersion, and lower volume of limbic tracts were found, particularly for the fornix, cingulum and medial forebrain bundle. Associations were found between limbic tract microstructure and volume, particularly of the cingulum, uncinate fasciculus and anterior thalamic radiation, and memory, learning, behavioural and emotional functioning. This study improves knowledge of the contributing factors to poor neurodevelopmental outcomes in preterm children.
Introduction
Infants born very preterm (VPT, <32 weeks’ gestation) are at high risk compared with infants born full-term (FT, ≥37 weeks’ gestation) of having problems later in life in wide-ranging neurodevelopmental domains. Neurodevelopmental delays have been reported in VPT children in memory, learning, emotion and behaviour,1,2 which are considered key functions of the brain’s limbic system.3 The current study aimed to characterise the major white matter fibre tracts in the limbic system in VPT compared with FT children at 7 years of age, and to investigate whether limbic tracts are associated with concurrent neurodevelopmental outcomes in VPT children.Methods
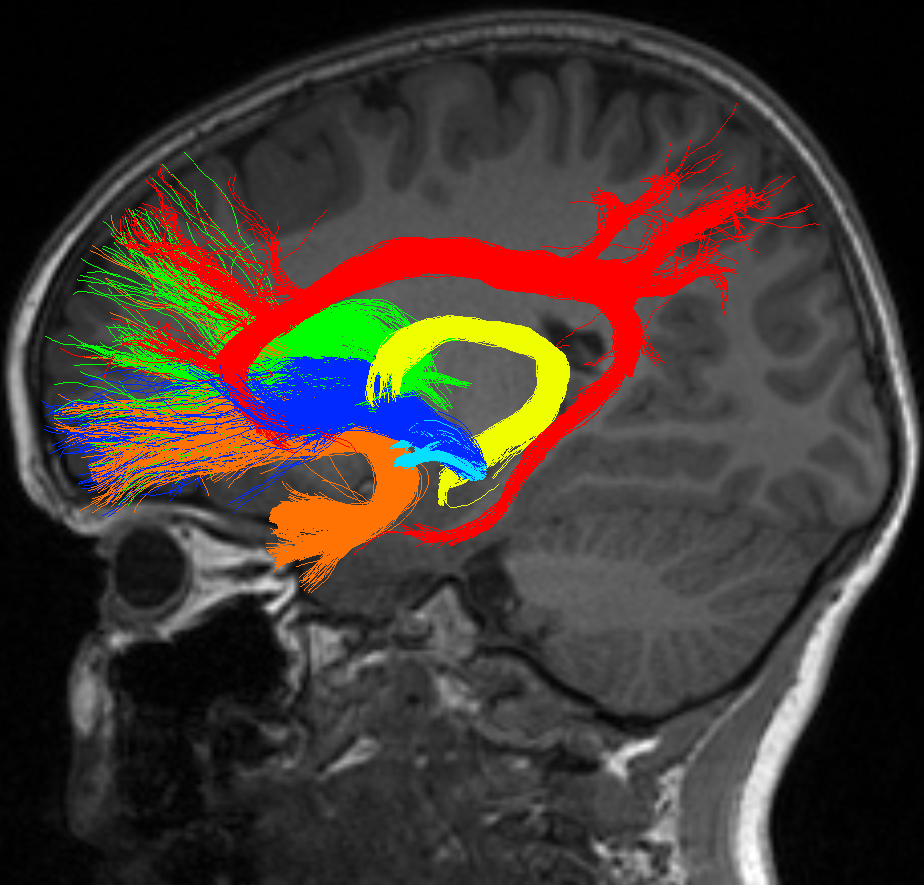
224 VPT (<30 weeks’ gestation and/or <1250g birthweight) and 46 FT (≥37 week’ gestation) infants were recruited during the neonatal period into a prospective longitudinal study, of which 198 VPT and 43 FT children attended a 7-year follow-up study, and 144 VPT and 33 FT children were included in the current study (exclusions were due to incomplete diffusion acquisitions or poor image quality). Diffusion magnetic resonance (MR) images were acquired (sequence 1: b= 1200 s/mm2, 25 gradient directions; sequence 2: b= 3000 s/mm2, 45 gradient directions). Several of the main tracts in the limbic system were delineated using probabilistic constrained spherical deconvolution (CSD)4 tractography by operators with specific relevant knowledge: cingulum A.M.; fornix T.N.; uncinate fasciculus C.K.; medial forebrain bundle including superior-lateral and inferior-medial branches J.P.; anterior thalamic radiation M.C. (Figure 1). Diffusion tensor imaging (DTI) and Neurite Orientation Dispersion and Density Imaging (NODDI)5 measures were extracted from tracts and tract volumes were calculated. Neurodevelopmental outcomes assessed included verbal memory and learning (California Verbal Learning Task, Children’s Version – list A total trials 1-5 scaled score), visual memory and learning (Children’s Memory Scale – long delay scaled score), working memory (Working Memory Test Battery for Children- backwards digits recall scaled score) and behavioural and emotional problems (Strengths and Difficulties Questionnaire – total score). IQ was also assessed in the current study as previous studies have found associations between limbic structures such as the hippocampus and general cognition in VPT children.6 Linear regressions, fitted using generalised estimating equations to allow for multiple births, were used to (i) compare tract measures between VPT and FT groups, and (ii) explore associations between tract measures and neurodevelopmental outcomes. Analyses were adjusted for age, and tract volume analyses were performed with and without adjusting for intracranial volume (ICV).Results
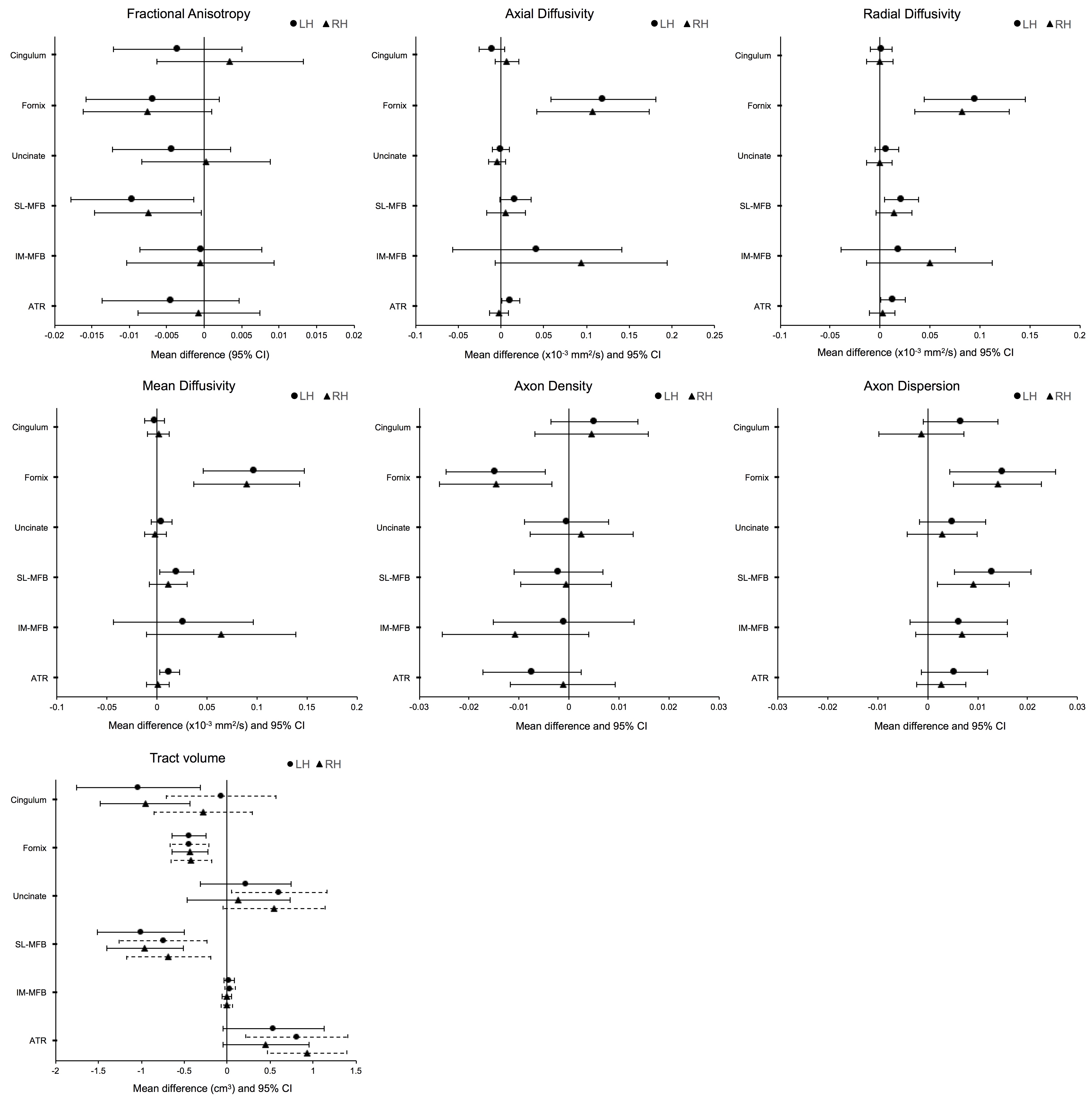
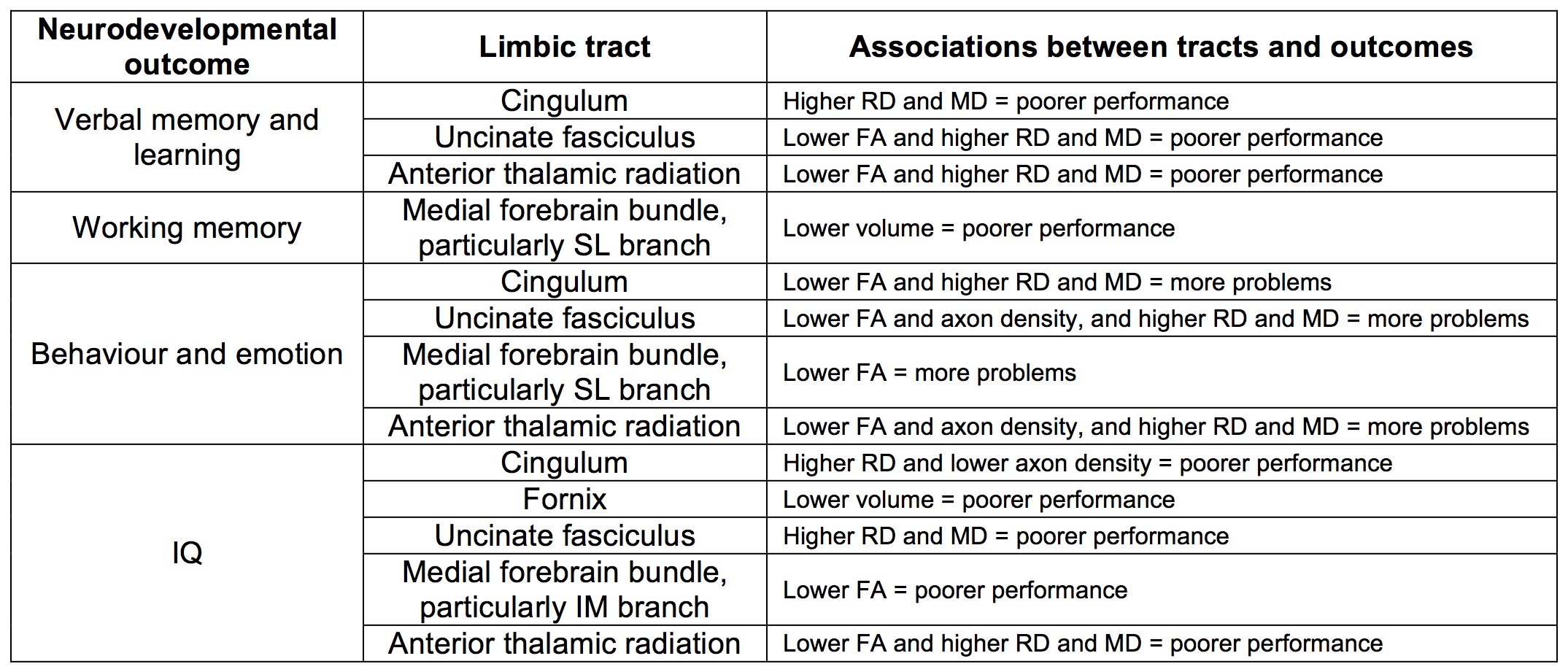
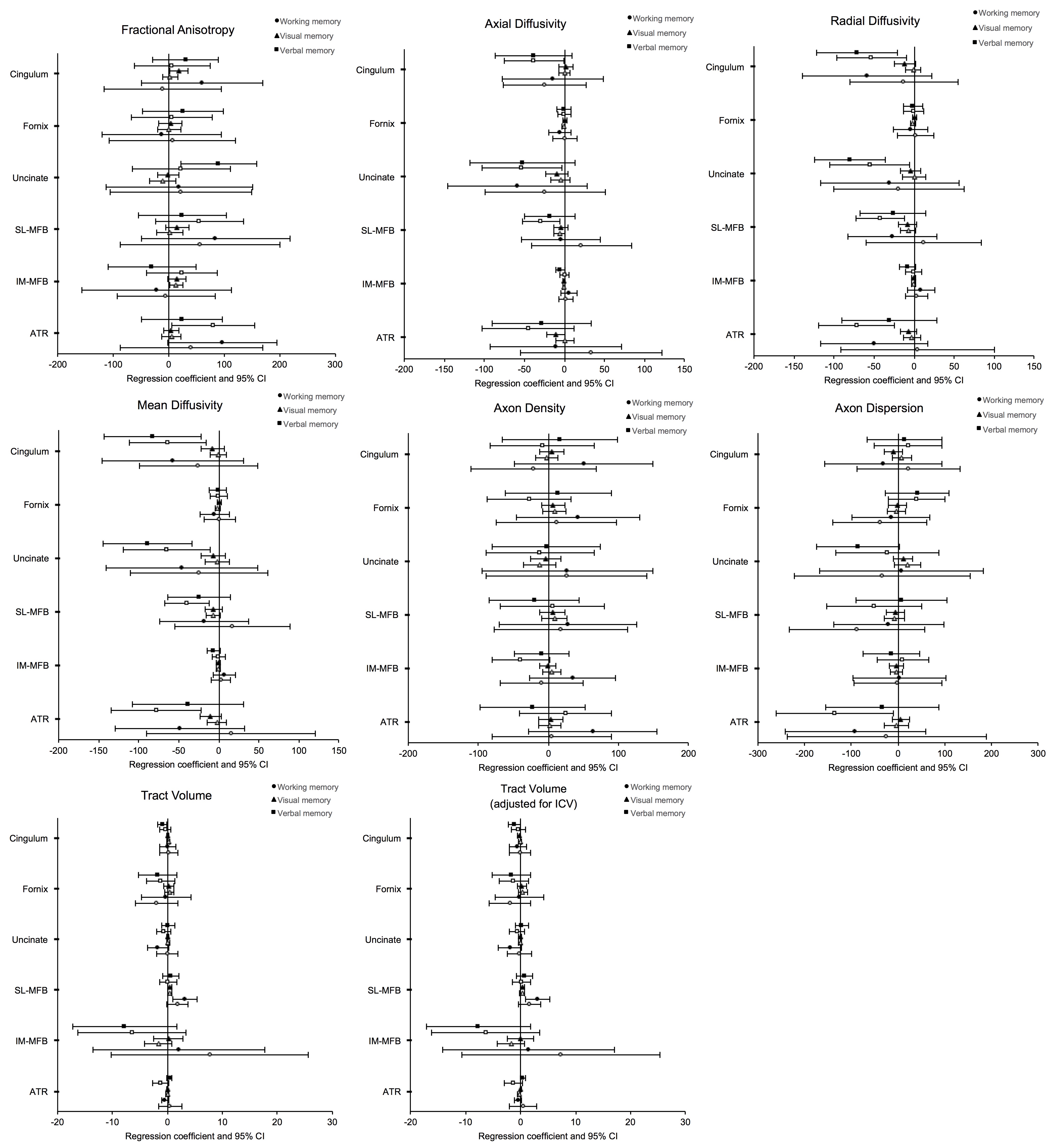
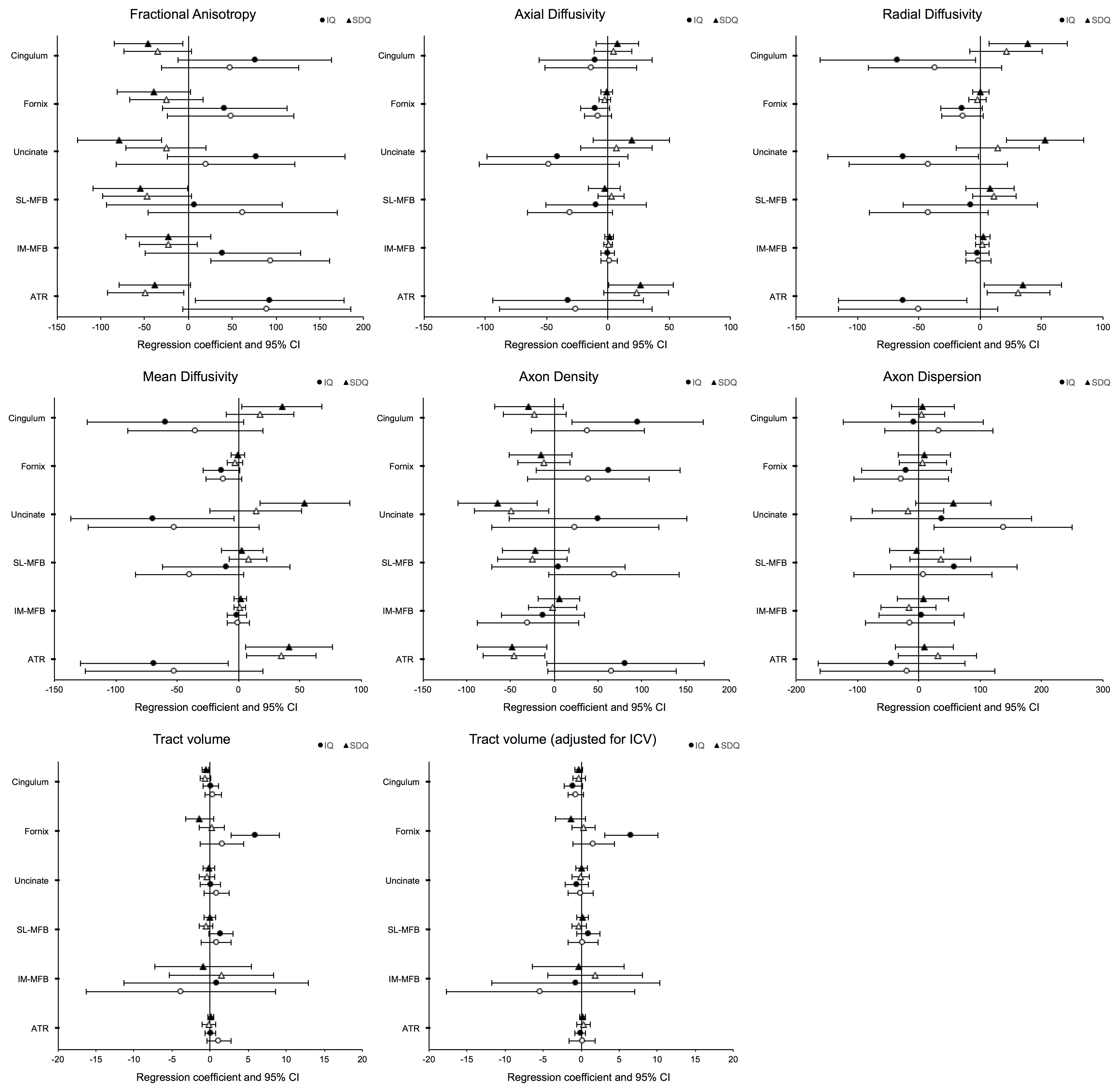
There was evidence for differences in tract measures in VPT compared with FT children. In particular, the fornix had lower fractional anisotropy (FA), axon density and volume, and higher diffusivities and axon dispersion; the medial forebrain bundle had lower FA and volume and higher axon dispersion; the cingulum had lower volume, although this weakened after adjusting for ICV (Figure 2). There was also evidence for associations between several tract measures and neurodevelopmental outcomes. The main tract-function associations are summarised in Table 1. Regression coefficients and 95% confidence intervals for all associations are plotted in Figures 3 and 4, to aid interpretation of the strength and magnitude of the associations.Discussion
Volume and microstructure of limbic tracts differed between VPT and FT children, particularly for the fornix, as well as the medial forebrain bundle and cingulum. This suggests that VPT birth leads to delayed or disrupted limbic system development in childhood, with possible axonal changes such as lower density (possibly reflecting axon loss, increased space between axons, or decreased myelination) and higher dispersion (possibly reflecting less coherently organised axons). Several associations were identified between limbic tracts, particularly the cingulum, uncinate fasciculus and anterior thalamic radiation, and outcomes in cognition, memory, emotion and behaviour. These findings support the view that the limbic tracts have a role in these functions, and suggest that microstructural alterations to these limbic tracts may have affected performance in these functions in VPT children.Conclusion
The current study is the first to investigate the network of major limbic fibre tracts in children born preterm. This study improves knowledge of the brain structural changes underlying neurodevelopmental functioning, particularly memory and behaviour, in VPT children. The next step is to use predictive statistical modelling to identify individual children who are at risk of poor outcomes and would benefit from close monitoring and early intervention.Acknowledgements
No acknowledgement found.References
1. Omizzolo C, Scratch SE, Stargatt R, et al. Neonatal brain abnormalities and memory and learning outcomes at 7 years in children born very preterm. Memory. 2014;22(6):605-615.
2. Treyvaud K, Doyle LW, Lee KJ, et al. Social-emotional difficulties in very preterm and term 2 year olds predict specific social-emotional problems at the age of 5 years. J Pediatr Psychol. 2012;37(7):779-785.
3. Catani M, Dell'acqua F, Thiebaut de Schotten M. A revised limbic system model for memory, emotion and behaviour. Neurosci Biobehav Rev. 2013;37(8):1724-1737.
4. Tournier JD, Calamante F, Connelly A. Robust determination of the fibre orientation distribution in diffusion MRI: non-negativity constrained super-resolved spherical deconvolution. Neuroimage. 2007;35(4):1459-72.
5. Zhang H, Schneider T, Wheeler-Kingshott CA, et al. NODDI: practical in vivo neurite orientation dispersion and density imaging of the human brain. Neuroimage. 2012;61(4):1000-1016.
6. Thompson DK, Wood SJ, Doyle LW, et al. Neonate hippocampal volumes: prematurity, perinatal predictors, and 2-year outcome. Ann Neurol. 2008;63(5):642-651.
Figures