0870
The clinical evaluation of combining DWIBS with whole body T1w imaging for diagnosing bone marrow involvement in lymphoma patients: a comparison with PET/CT1The First Affiliated Hospital of Zhengzhou University, 1st, Zhengzhou, People's Republic of China, 2Philips Healthcare, Beijing, People's Republic of China
Synopsis
This study aimed to evaluate the value of the combination of DWIBS (diffusion weighted imaging with background signal suppression) with whole body T1w imaging for diagnosing bone marrow involvement (BMI) in lymphoma patients, compared to PET/CT imaging. In the first part of this study, patients with newly diagnosed lymphoma were includedand whole body DWIBS, T1w and PET/CT images were acquired for all 20 subjects. For the assessment of individual lesions, DWIBS with whole body T1w has advantages over DWIBS and has similar ability with PET/CT to detect BMI lesions.
Abstract
Purpose: To evaluate the clinical value of the combining of DWIBS (diffusion weighted imaging with background signal suppression) with whole body T1w imaging for diagnosing bone marrow involvement (BMI) in lymphoma patients, compared to PET/CT imaging.
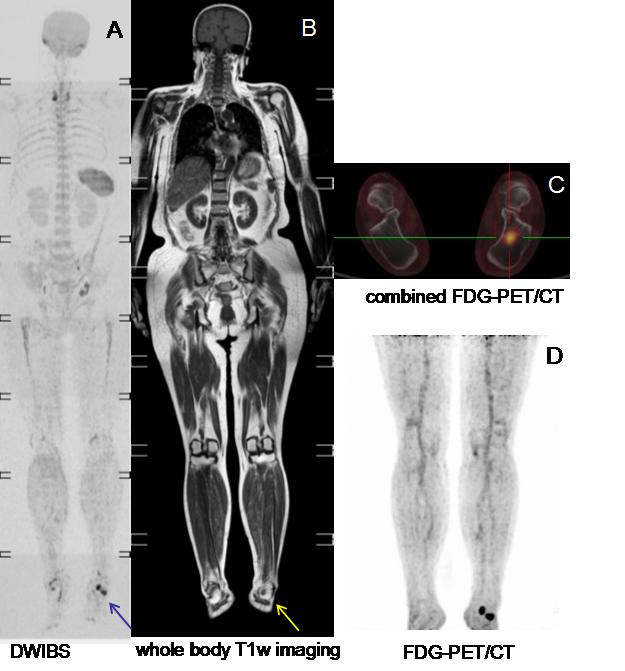
Materials and Methods: Patients with newly diagnosed lymphoma were included in this study and whole body DWIBS, T1w and PET/CT images were acquired (as shown in Figure 1). MRI images were acquired by using a 1.5T MR scanner (Achieva Intera, Philips, the Netherlands) with the following parameters. DWIBS: STIR-EPI, axial acquisition, TR=2996ms, TE=67ms, TI=180ms, FOV=530 mm×349mm×240mm for each station, slice thickness=6mm, b value=0 and 800s/mm2 , scan time=15min for 8 stations; whole body T1w: coronal acquisition, TR=0.99ms, TE=17.5ms, FOV=530mm×265mm×209mm for each station, slice thickness=6mm, scan time=10min for 8 stations. Clinical evaluation of the all the images were performed by 2 radiologists (especially for MR) and 1 nuclear medicine physician (especially for PET/CT) independently. BMI diagnosis was determinated if one of the below conditions was satisfied: 1, Results of the bone marrow biopsy was positive; 2,Results of both PET/CT and DWIBS were positive; 3, Results of only PET/CT or MR showed BMI characteristics but BMI lesion vanished after the treatment of the tumor. Chi-square test (there is a statistical difference when p<0.05) was performed to compare the sensitivity and specificity between different diagnosis methods. ROC analysis was carried out to evaluate the performance of the three diagnosis methods. All the statistical analysis was performed with SAS 9.3 software.
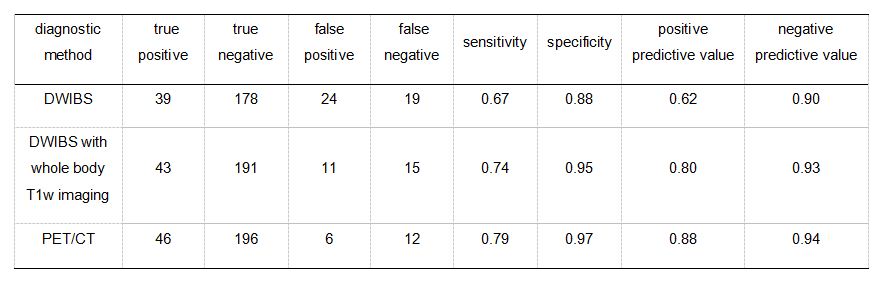
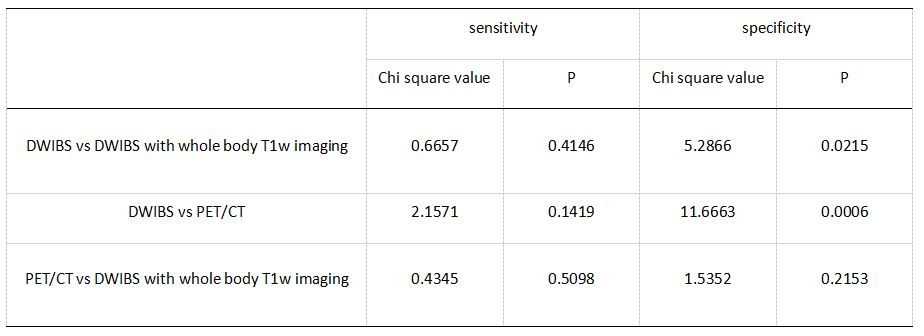
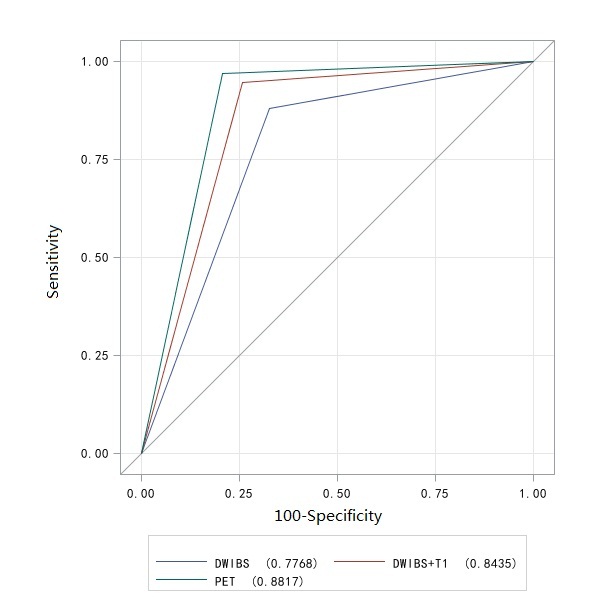
Results: The skeletal system was classified into 13 anatomic regions and assessed for the presence of BMI. BMI was confirmed in 58 regions of 18 patients. Table 1 shows the BMI diagnostic results with DWIBS, DWIBS combining whole body T1w and PET/CT. There is no significant difference (Chi square test, p>0.05) on the sensitivity of DWIBS, DWIBS combining whole body T1w and PET/CT. There is a significant difference (Chi square value=11.67, p<0.001) on the specificity between DWIBS and PET/CT and no difference (Chi square value=1.54, p>0.05) between DWIBS with whole body T1w and PET/CT(Table 2). The ROC analysis results are showed in Figure 2.
Discussion: DWIBS can improve MRI imaging contrast especially for total body lesions, but the image resolution was decreased for compensation for the scanning time and signal-to-noise ratio (SNR)[1].And the images are usually affected by various artifacts caused by magnetic susceptibility inhomogeneous and motion[2]. In this work, a combination of DWIBS and whole body coronal T1w was applied to evaluate the infiltration and distribution of BMI. Compared to DWIBS only, it showed a better lesion location, diagnosis accuracy and evaluation efficiency. Compared to PET/CT, DWIBS and T1w imaging have no radiation effects but with similar diagnosis ability[3]. In addition, the scanning for both DWIBS and T1w can be completed within 30mins, which is available in conventional clinical application.
Conclusion: The combination of DWIBS with T1w imaging can improve the ability of detecting BMI in lymphoma patients compared to DWIBS only. And it has the similar diagnostic ability compared to PET/CT imaging.
Acknowledgements
We thank Zhuo zhi zheng for assistance with the experimentsReferences
[1] Fischer MA, Nanz D, Hany T, et al. Diagnostic accuracy of whole-body MRI/DWI image fusion for detection of malignant tumours: a comparisonwith PET/CT[J]. Eur Radiol, 2011, 21(2):246-255.
[2] Gatidis S, Schmidt H, Martirosian P, et al. Apparent diffusion coefficient-dependent voxelwise computed diffusion-weighted imaging: An approach for improving SNR and reducing T2 shine-through effects[J]. J Magn Reson Imaging, 2016, 43(4):824-832.
[3] Albano D, Patti C, La Grutta L, et al. Comparison between whole-body MRI with diffusion-weighted imaging and PET/CT in staging newly diagnosedFDG-avid lymphomas[J]. Eur J Radiol, 2016, 85(2):313-318.
Figures